"They have behaviour, we have relationships?"
Greenhill, B., 2011. "They have behaviour, we have relationships?". Reformulation, Winter, pp.10-15.
Using CAT to understand why the “Un-offered Chair” remains un-offered to People with Learning Disabilities
“At a fundamental level, working with a person with a learning disability in psychotherapy is the same as working with anyone else, and as different. They [sic] are often not seen as suitable for treatment, but here it is psychotherapy that is handicapped” (Linington, 2002)
Introduction
Bender’s (1993) concept of the “un-offered chair” remains a striking metaphor for the negative attitudes of psychotherapists towards psychotherapy with people with the label of “learning disability” (LD). In this essay I will attempt to outline how CAT might help to formulate practitioner’s resistance to understanding the emotional difficulties of people with learning disabilities in relational terms both in therapeutic work with the service user and systemic behavioural work. Drawing on the work of King (2005) and Psaila and Crowley (2006), I hope firstly to explore why there may be reluctance of many psychotherapists to work with disability. Secondly, despite the early promise behaviourism and learning theory offered in “educating the ineducable”, the notion of a humane behaviourism can sometimes seem lost in the long running, increasingly polarised debates between behaviourists and psychotherapists.
Rather than accepting what is sometimes interpreted as the therapeutic pessimism of the behavioural approach, I hope to suggest that CAT offers an opportunity both to reformulate our understanding of “learning disability” and to reformulate behavioural approaches in a more emotionally resonant and relational context (Moss, 2006; Bancroft et al., 2008; Lloyd and Williams, 2003). In structuring the essay, I will use Psaila and Crowley’s (2006) research on commonly occurring reciprocal roles in work with people with a learning disability to try to understand the function of this reluctance to engage from the therapist’s perspective. Amongst these are: “rejecting to rejected”, “controlling to controlled” and “contemptuous to contemptible” (see also Lloyd and Williams, 2003).
“Challenging Behaviour” - “Rejecting to Rejected”
Despite an elevated incidence of mental health difficulties relative to the general population (Dosen & Day, 2001) and a well documented ability to self-report (Lindsay et. al., 1994; Stenfert-Kroese et. al., 1996) people with the label of a learning disability still have little access to therapy (Stavrakaki & Klein, 1986; Hurley, 1989; Butz et. al., 2000; Dodd & McGinnity, 2003; Johnson et. al., 2003; Lynch, 2004). Instead, services to people with this label continue to demonstrate an over-reliance on an “unholy trinity” of behaviour modification, medication and cognitive assessment (Hurley, 1998).
Various attempts have been made to account for why therapy is still not seen as a particularly viable way of engaging with the emotional and relational difficulties of people with a learning disability. Explanations range from those locating the problem within the damaging institutionalisation of people with a learning disability such that they have been “out of sight and out of mind” for decades (Arthur, 2003) to those suggesting the exclusion results from a focus on the needs of the service provider, rather than the service user (Waitman and Reynolds, 1992). Both explanations seem to point to something deeper about society’s relationship to disability which, in turn, impacts upon the way in which, as CAT therapists, we do, or don’t, dialogically engage with the relational difficulties of learning disabled people.
In my work in specialist learning disability services, colleagues and I have often queried the emotional functionality for staff of barriers which exist to therapy for learning disabled people. Whether barriers emerge from target driven practice and the need to reduce waiting lists, to “get through-put”, lack of training, or the way in which referrers construct a person’s difficulties, there seems to be much more comfort for practitioners in understanding distress as behaviour or through diagnosis, than in connecting with the way any of us might feel if we lived the life of the person in front of us.
Much of the literature on psychological intervention for people with the label of learning disability is organised around the concept of “challenging behaviour”. Originally conceived as a term recognising that unmet need may manifest in a person’s behaviours which then pose a challenge to services, “challenging behaviour” is often viewed as a “manifestation of psychopathological processes”. The result is that “people with learning disabilities who present behavioural challenges are often marginalised, stigmatised, disempowered and excluded from mainstream society” (Royal College of Psychiatrists, 2007)
Such exclusions from local services may take the form of “out of area” placements (Mansell, 1993; 2007) where the person is placed away from their family and their community. These exclusions may involve not receiving day services, employment opportunities, education or adequate mainstream healthcare (Mencap, 2007). They may also involve service responses which include seclusion, restraint, locked doors, and, as evidenced by the scandals of Winterbourne, Sutton and Merton or Cornwall, may give rise to abuse. Interventions may take the form of inappropriate prescribing, risk avoidance rather than risk management and punitive and aversive behavioural treatment (Royal College of Psychiatrists, 2007).
Behaviourism: “Controlling to Controlled/Compliant”
“We undertake to predict and control the behaviour of the individual organism”
(Skinner 1953).
Lovett (1996) rightly notes that at its outset, the application of behavioural approaches with people with a learning disability was an innovative and positive step. People with learning disability within the institutions were scarcely seen as human, with one commentator apologising for “anthropomorphisising” people with the label of disabilities. In this context, the ideas that firstly those with learning disabilities are people, and secondly that education was a possibility, were progressive. However, “what began as a technique for teaching, rapidly became a technique for controlling” (Lovett, p68). Over time there may have been increasing focus on reward (“token economies” and “star charts”) rather than on aversive techniques (pain), but as Lovett notes “until people with learning disabilities are in a position to decline these therapies, no amount of sophistication will remove the elements of control and coercion implicit in the theory supporting these practices”.
Whilst the debate about the effectiveness of different therapies has raged since psychotherapy began, Sturmey’s (2005) comments deeply polarised opinion within the field of learning disabilities. In a controversial article, Sturmey aimed to summarise the evidence base regarding intervention frameworks for people with a learning disability. Sturmey argues given the lack of published evidence relating to the effectiveness of psychotherapy with people with a learning disability, psychotherapy should not be practised at all. He states, “We are unable to make any conclusions as to the effectiveness, ineffectiveness, or harmful effects of psychotherapy based on the scientific evidence… given the hundreds of studies documenting the effectiveness and efficiency of behavioural interventions, behavioural approaches behavioural approaches must remain the preferred treatment option for people with mental retardation”.
In contrast, Beail and (many) others (2005) argue vociferously that “people with mental retardation have a right to a similar range of therapies that are used in the general population”. Beail notes Sturmey is right in asserting there is a lack of evidence for non-behavioural interventions but that “there is no room for complacency with regard to the evidence base for behavioral interventions”. Further, that most of the interventions Sturmey describes have been carried out in “non-integrated settings”.
Within the field of learning disability there has been a different approach to people’s challenges, perhaps best exemplified by the work of both Lovett (1996) and Pitonyak (2002). Both begin to offer a relational understanding of challenging behaviour. Pitonyak’s central idea is that “all behaviour is a communication”, or in his words is “meaningful”, and that the task of intervention is to encourage supporters of the person to listen to the function of difficult behaviours. In “Learning to Listen”, Lovett acknowledges that the relational function for many practitioners of behavioural assessment is distancing; “Most of what passes as assessment seems to be denial about the mutuality of our common condition”.
Behaviourism’s dominance, is perhaps functional from the point of view of practitioners seeking to minimise their engagement with the difference of learning disability and the discomfort experienced by the “perceived lack” many associate with learning disability. It is just one example of how practitioners collude with the common reciprocal roles of people with learning disability. Again, Lovett notes (p228) “service systems…almost invariably imitate the people they attempt to serve. People who are dangerously aggressive tend to attract services that act out violently. Similarly, if a person hurts himself by banging his head…the team members often act as if they were the ones insensitive to pain. With no irony whatever, they may decide that the first thing they have to do is establish a baseline…a group of ordinary people would be far more likely to decide that the first thing to do is to protect the person’s head…”.
Psychotherapy and Learning Disability: ‘Contemptuous to Contemptible’?
In his article tracing “the history of therapeutic disdain towards people with a learning difficulty”, Bender discusses the apparent prejudice of mental health professionals towards therapy with learning disabled people. After exploring Freud’s attitudes to “those patients who do not possess a reasonable degree of education”, he describes the “psychotherapeutic neglect” of people with a learning disability by Freud’s “followers” based on their selective reading of Freud’s early work. Bender writes, “the simplest explanation appears to be that psychoanalysts framed rules of exclusion to remove the less attractive of those needing help with little or any respect of the evidence relating to these exclusions”. Bender finds similar prejudice in Carl Roger’s inability to engage with “the unattractively distressed”.
The same desire of therapists to distance, also features in Bender’s account of behaviour therapy. Bender describes two modes of delivery within the behaviourist school. In the first of these, techniques such as behavioural flooding and graded desensitisation, derived from Pavlovian drive theories of learning, are applied within a therapeutic process, or at least with the person concerned being present. In the second, Skinnerian, mode, which became dominant, the person was not required to take an active role as the focus was on environmental manipulation. Skinner’s “black box” approach to mental processes meant that changing the contingencies of behaviour became the aim of intervention and “the subjective awareness of the patient was either irrelevant, or at best, another piece of information to be gathered”. Bender argues that as a result there was little development in psychodynamic therapies for people with the label of learning disability until the 1980’s.
Reformulating Learning Disability
The dominant understanding of learning disability within services relies heavily on the concept of intelligence, usually framed very narrowly as cognitive intelligence and heavily influenced by Piaget. There are a number of issues with this understanding, which result perhaps in a quite un-CAT like formulation of people with learning disability and an over-reliance on cognitive abilities per se to predict a person’s capacity to engage in the therapeutic alliance. Firstly, this view reifies intelligence as a property of individual’s minds rather placing it within a relational space. Secondly, it underplays the impact of attachment theory. Finally, it doesn’t really allow for other human qualities, “emotional intelligence” (Sinason, 1992) for example, to shape experience and permit potential to change.
Ryle and Kerr (2004) argue that we are “people whose nature it was to be formed by nurture” (p23). Although biology undoubtedly plays a role in our being in the world, so much of this is shaped by the subtle forces of other people’s expectations, social roles and relationships. Ryle quotes Eisenberg, who states, “Major brain pathways are specified by the genome; detailed connections are fashioned by, and consequently reflect, socially mediated experience”. In application to people with a learning disability, this resonates much more with the so-called “social” rather than “medical” model of disability.
Traditionally, psychologists dissect intellect through “subtests” of cognitive performance, attributing deficits solely to the mind and functioning of the tested person. For Vygotsky (1978), intelligence exists in the dialogue between two people, becoming internalised and then coming back into the dialogue. In child development, the inter-psychic becomes the intra-psychic as speech is internalised. As we test out our understandings of ourselves and our identity in the world, this is refracted back to us by the relationships around us. When our existence is reflected back to us tinged with contempt, disappointment, distance or not at all, it has a profound effect on identity.
Much of the literature concerning early attachment and learning disability focuses on the way in which social understandings of disability give rise to emotional distancing by parents. Niedecken’s (2003) thesis, for example, is that people with learning disabilities are damaged by the negative messages parents receive when they are born. These are then transferred to the infant by the parents in early socialization. A similar notion is found in Sinason’s (1992) work, although the two authors differ regarding primary and secondary aspects of disability. Sinason builds on Freud’s concept of “secondary gain”, introducing the term “secondary handicap” to describe the need of the person with a learning disability to separate themselves from the pain of abuse; crudely put, “better to be stupid than to be in pain”. If this is where early patterns of relating and reciprocal roles are established for people with a learning disability the effects are potentially limiting.
Psaila & Crowley (2006) suggest people with learning disability seem to have fewer reciprocal roles than some other social groups. It has been suggested that this may be due to increased dependence on other people and services leading to a less robust sense of a person’s own identity. The impact of trauma, may lead to restricted repertoire of reciprocal roles (Ryle, 1999), either in this case as result of the social meaning of disability itself or resulting from increased vulnerability from sexual or other abuse. Infantilisation, being treated as child-like and becoming stuck in this role may further restrict the reciprocal roles of a person with learning disability (see also King 2005).
There is also a possibility that stereotypes, manifest in our relationships to people with learning disabilities as parents, colleagues, workers and therapists restrict the roles that are available. It might be argued that the most limiting and constraining force on people with learning disability is the societal and relational constriction of their roles, behaviours, and their voice rather than “natural” ability. In an interesting paper on Autism, Lloyd and Potter (in preparation) describe a multifaceted model of intelligence where various intelligences including “social intelligence” define our abilities to function in the world. Perhaps as a society we do not give permission for people with learning disabilities to occupy the full breadth of the relational space which might ameliorate any “organic” difficulty.
Exits: ‘A therapy like any other?’
King (2005) argues that for almost all people with a learning disability it is possible to forge a meaningful emotional connection but that there are particular issues in the therapeutic relationship which it is important to address. As we are drawn into procedures with a learning disabled person powerful feelings of guilt & intense compassion (Sinason, 1992), contempt (Symington, 1992) and the desire to deny disability through avoidance, distancing and rejection may emerge. King argues that working with people carrying the “woundedness & weakness” of disability necessitates being able to face these things in ourselves. It is striking that many black practitioners, gay practitioners and other “diverse” workers, are attracted to learning disability services, almost as if in rescuing our clients, we can rescue the wounded aspects of ourselves.
King’s construction emphasises mindfulness of processes within therapy and avoiding collusion. She describes a “developmentally needed or reparative relationship” in response to deficiencies in original parenting. For King, three types of injury or deficit; trauma (e.g. abuse), strain (e.g. negative societal attitudes) and extra-familial limitations or tragedies (e.g. genetic conditions), require a therapeutic emphasis on witness, containment, and care. Where there is evidence of neglect there may be a need for careful attention and responsiveness. Conversely, where smothering and overprotection feature highly in the person’s transference and history, there may be a need for respect and space. In CAT terms, a deliberate use of positive reciprocal roles in therapy may provide a “reparative holding environment for both patient & therapist”. However, she states that “getting stuck” in the reparative relationship may foster dependency and infantilisation.
King suggests that an aim of individual therapy may be to move from the “reparative” towards a deeper “person to person” relationship. Mindful of stereotyped relating, the therapist aims to foster more flexibility and human connection which “may include certain well timed self disclosures by therapist”, at the same time “acknowledging the difference in intellectual abilities between service user and therapist”. King surmises “perhaps what people with a learning disability most long for is the experience of a person-to-person relationship in which two adults meet as equals”. If our value is not defined by intellectual capacity then equal but different is possible.
Exits: The dialogic function of “behaviour”
CAT’s potential to understand aspects of relating on many levels offers a useful “exit” to the snags involved in understandings which distance us from the pain of disability, especially when that pain is communicated through violent behaviours to the self or other. It is tempting, when faced with sheaths of “incident forms” describing assaults, self injury and abuse, to revert to a “functional analysis” of a person’s behaviours. The frequency data is entered, the graphs compiled, the formulation constructed and the management strategies are prepared, usually to be delivered to staff supporting the person. We absent the person and cleanse the relational from the process under the guise of being objective, “scientist-practitioner” clinicians.
Moss (2006), in a paper discussing the application of CAT to work with clients with learning disabilities, notes that not only verbal dialogue but “gesture, drawing and other non-verbal signs” can be understood “as a ‘way in’ to the individual’s subjective experience”. This is implicit in “Change for the Better” (McCormick, 2002) which suggests that working with images and painting, modelling, or cutting out pictures for example of dilemmas: “either I’m a battering ram or modelling clay” can be a powerful therapeutic tool. In my own practice, I have found working with people through line drawings of relational roles and picking objects from a box (stones, beads, shells) to represent the self, others, or a trap or dilemma to be effective ways of representing relationships when they cannot be conveyed through speech.
Moss goes on to argue in as much as gestures constitute a sign, that “the triggers and consequences of challenging behaviour can…be conceptualised as reciprocal role procedures between the client and their support system, namely around issues of control and punishment”. Bancroft et al (2008), reflecting on discussions at the ACAT Learning Disability Special Interest Group, have also begun describing behaviourist ideas within a CAT paradigm. They state that reciprocal roles have an approximation to the behavioural concepts of “mutual stimulus and response”. Crucially, they also state that “whereas in behavioural terms we refer to ABCs (Antecedent, Behaviour and Consequence), in CAT we find a similar account in one of the procedural sequences described as a trap” (p.23). Lloyd and William’s (2003) contribution to the understanding challenging behaviour in CAT terms focuses on staff’s emotional responses to behaviours; formulating the relational in people’s challenges may open up less self-defeating ways for staff to engage.
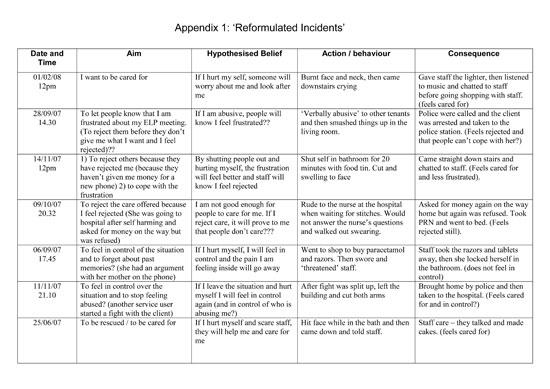
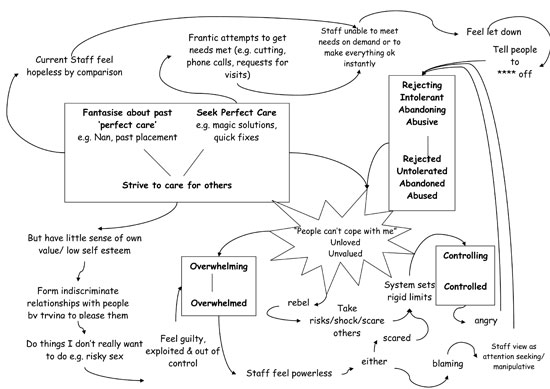
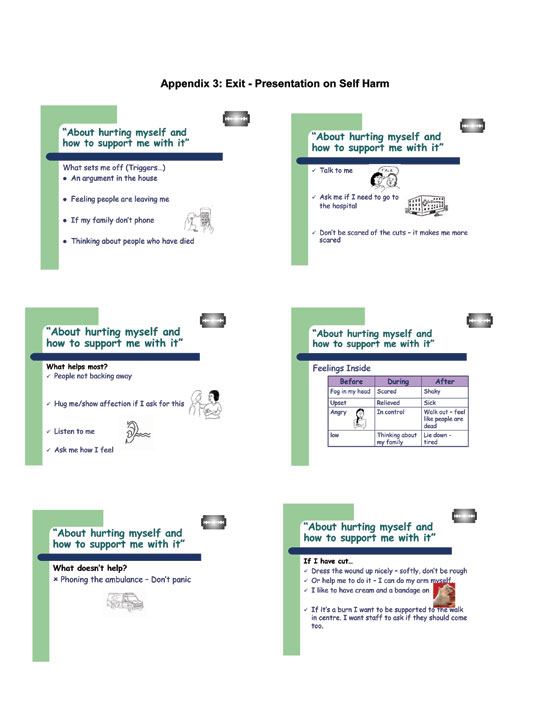
Appendix one contains an attempt to reformulate a functional analysis of a young woman with learning disability in CAT terms. The “reformulated incidents” (appendix 1) and contextual reformulation (appendix 2) were used in training with her staff team. Contextual reformulation may enable staff supporting people with a learning disability to understand the person, and their own reactions in a less distancing, more relational way. Ryle & Kerr (2004) highlight the potential role of CAT “as a consultative tool” for working with staff who support people with learning disabilities “both in residential and community settings to help them in avoiding collusion with clients’ maladaptive RRP’s” (see also Clayton, 2001). Sometimes it can be difficult to construct the boundaries around such work, but as Bancroft et. al. (2008) state, “If the client can performs some of the therapist’s ‘relating to the team duties’ such as when the client rather than the therapist tells the team about their diagram, the power belongs to the client within in their orbit”. Whilst this was not entirely possible in this instance, the young woman was able to deliver training around her exits by informing staff, in an accessible way about helpful and unhelpful responses to her self harm (appendix 3).
In my own work, as a practitioner with people with learning disabilities, I have felt the pull of some of the roles Psaila and Crowley (2005) describe. Perhaps the most painful aspect of this is compiling the history which forms the basis of functional analysis having spent time with the person. Often, people with learning disabilities and complex needs have horrific abuse histories. They may not be able to articulate their experiences in a way which their workers can understand. It may be shown in the scars on the person’s body and their behaviours, but is all too often hidden by “the handicapped smile”. Whilst there can be boundary issues in occupying multiple roles (that of “care coordinator” and “therapist”), working within a CAT framework has helped give me a framework for my practice so that the person can be more relationally understood and empowered within their systems. This seems to have more meaning and power for the person, professionals and support staff.
I am mindful in writing this essay that the “common idealised reciprocal roles” Psaila and Crowley (2005) identify, (“rescuing/caring to rescued/cared for” and “special/perfect to learning disabled”) may have a role in producing an “intellectually striving” account which suggests CAT as a panacea for all. Hopefully, my account is neither distancing nor an attempt to rescue by wishing for a “cure” for disability, “if only we got our interventions right”. If, as therapists, we are more able to offer the therapeutic chair to people with a disability, I believe it enriches our understanding of our own “good enough” humanity and our own differences, however painful at times these may be.
Summary and Conclusion
This essay has argued that it is simplistic to argue behaviourism remains the “treatment of choice” for people with the label of learning disability solely because of the weight of empirical evidence. It also serves an emotional function. As practitioners and researchers we often occupy unhelpful reciprocal roles in relation to “learning disability”. This leaves the therapeutic chair all too often un-offered to learning disabled people, who even within the world of CAT, are frequently seen as cognitively unable to collaborate in therapy. I have quoted King below as I believe she puts the reasons for this extremely eloquently. I share her optimism that, if we are open to the vulnerability in ourselves, working with people labelled with learning disability can be rewarding and feel that the flexible and integrative nature of CAT can provide a bridge between behavioural and relational approaches to work with people with learning disabilities.
“As individuals, as psychotherapists and as a society, it is healthier to learn to connect with people with a learning disability and the pain they bear for us, and the gifts they bring us, than it is to distance ourselves or destroy. In wishing to conceal or get rid of disability we deny or destroy an essential part of our humanity. Living in a society which places such a premium on achievements, possessions and the perfect looks of the adverts, it may be hard to be in touch with the imperfections which are part and parcel of the human condition. Connecting with disability brings us more in touch with the whole of ourselves, allowing us, if we will, to accept the strengths and weaknesses of our full humanity”(King, 2005)
References
Arthur A. R. (2003) The emotional lives of people with intellectual disabilities. British Journal of Learning Disabilities 31, 25–30.
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, K., Lloyd, J., & Murphy, N. (2008). Is CAT an Island or a Solar System? The dilemmas in the frame when working with people in learning disabilities services. Reformulation, Issue 30, Summer, 23-26.
Bender, M. (1993). The unoffered chair: the history of therapeutic distain towards people with a learning difficulty. Clinical Psychology Forum, 54, 7 – 12.
Beail, N. (2005) Responses to Sturmey (2005) on psychotherapy: Evidence base for behavioral interventions: Critical commentary. Mental Retardation, December 2005, vol. 43/6, 442-445.
Butz, M. R., Bowling J. B. & Bliss C. A. (2000) Psychotherapy with the mentally retarded: a review of the literature and the implications. Professional Psychology: Research and Practice 31, 42–47.
Clayton, P. (2001). Using Cognitive Therapy in an institution to understand and help both client and staff. In Landsberg, G. & Smiley, A. (Eds.), Forensic Mental Health: Working with offenders with mental illness. 241-247. Kingston, NJ: Civic Research Institute
Department of Health. (1993). Services for people with learning disabilities and challenging behaviour or mental health needs. (The Mansell Report) London: Department of Health.
Department of Health. (2007). Services for people with learning disabilities and challenging behaviour or mental health needs: Report of a Project Group (Chairman: Prof J L Mansell). Revised Edition. London: Department of Health.
Dodd P. & McGinnity M. (2003) Psychotherapy and intellectual disabilities. Irish Journal of Psychological Medicine 20, 38–40.
Dosen A. & Day K. (2001) Epidemiology, aetiology and presentation of mental illness and behaviour disorders in persons with intellectual disabilities. In: Treating Mental Illness and Behavior Disorders in Children and Adults with Intellectual Disabilities (eds A. Dosen & K. Day), pp. 3–24. American Association Books, London.
Hurley A. (1989) Individual psychotherapy with mentally retarded individuals: a review and call for research. Research in Developmental Disabilities 10, 261–275.
Hurley A., Tomasulo D. J. & Pfadt A. G. (1998) Individual and group psychotherapy approaches for persons with intellectual disabilities and developmental disabilities. Journal of Developmental and Physical Disabilities 10, 365–386.
Johnson A., Mason H. & Withers P. (2003) ‘‘I might not know what you know but it doesn’t mean you can be awful to me’’. British Journal of Learning Disabilities 31, 31–36.
King, R. (2005). CAT, the therapeutic relationship and working with people with learning disability. Reformulation, June 2005.
Kroese, B.S., Dagnan, D., & Loumidis, K. (Eds.) (1997). Cognitive Behaviour Therapy for People with Learning Disabilities. London, Routledge.
Lindsay W. R., Michie A. M., Baty, F. J., Smith A. H. W. & Miller S. (1994) The consistency of reports about feelings and emotions from people with intellectual disability. Journal of Intellectual Disability Research 38, 61–66.
Linington, M. (2002). ‘Whose Handicap?’ Psychotherapy with people with learning disabilities. British Journal of Psychotherapy, 18 (3), 409-414.
Lloyd, J. and Williams, B., 2003. Reciprocal Roles and the ‘Unspeakable Known’: Exploring CAT within Services for People with Learning Disabilities. Reformulation Article, Summer 2003, 19-25.
Lynch C. (2004) Psychotherapy for persons with mental retardation. Mental Retardation 42, 399–405.
Lovett, H. (1996).Learning to Listen. Positive Approaches and People with Difficult Behaviours. London; Kingsley.
Moss, A. (2006). The Application of CAT to Working with People with Learning Disabilities. Reformulation, Summer, 20-27.
Neidecken, D. (2003). Nameless: Understanding Learning Disability. London, Routledge.
Pitonyak, D. (2005) ’10 Things you can do to support a person with difficult behaviours’, www.dimagine.com.
Psalia, C. & Crowley, V. (2005) CAT in PLD: An investigation into the common RR’s found within this client group. Mental Health and Learning Disabilities Research, 2005, 2, 96-108.
Royal College of Psychiatrists (2007). Challenging Behaviour: A Unified Approach. Clinical and service guidelines for supporting people who are at risk of receiving abusive or restrictive practices. College Report CR144. Royal College of Psychiatrists
Ryle, A. (1990). Cognitive Analytic Therapy: Active Participation in Charge. Chichester, Wiley.
Ryle, A. & Kerr, I. (2002). Introducing Cognitive Analytic Therapy: Principles and Practice. Chichester, Wiley.
Sinason, V.(1992). Mental Handicap and The Human Condition: New Approaches from the Tavistock. Free Association Books: London.
Skinner, B.F. (1953). Science and Human Behaviour. New York, Macmillan.
Stavrakaki C. & Klein J. (1986) Psychotherapies with the mentally retarded. Psychiatric Perspectives on Intellectual Disabilities 9, 733–743.
Sturmey, P. (2005) Against Psychotherapy With People Who Have Mental Retardation., Mental Retardation: Vol. 43, No. 1, pp. 55–57.
Symington, N. (1992) Countertransference with mentally handicapped clients. In: Psychotherapy and Mental Handicap (eds A. Waitman & S. Conboy-Hill), pp. 132–138. Sage Publications, London.
Vygotsky, L.S. (1978). Mind in Society: The Development of Higher Psychological Process. Cambridge MA: Harvard University Press.
Waitman, A. & Reynolds F. (1992) Demystifying traditional approaches to counselling and psychotherapy. In: Psychotherapy and Mental Handicap (eds. A. Waitman & S. Conboy-Hill), pp. 202–220. Sage Publications, London.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Greenhill, B., 2011. "They have behaviour, we have relationships?". Reformulation, Winter, pp.10-15.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities
Wells, S., 2009. A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities. Reformulation, Winter, pp.21-23.
Editorial
Lloyd, J., and Pollard, R., 2014. Editorial. Reformulation, Summer, pp.3-4.
Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group
Psaila, C.L. and Crowley, V., 2006. Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group. Reformulation, Winter, pp.5-11.
Trauma, Trauma and More Trauma: CAT and Trauma in Learning Disability
Julie Lloyd, 2019. Trauma, Trauma and More Trauma: CAT and Trauma in Learning Disability. Reformulation, Summer, pp.44-46.
When the therapist is disabled
Crowley, V., Field, B., Lloyd, J., Morrison, P., & Varela, J., 2014. When the therapist is disabled. Reformulation, Summer, pp.6-9.
Other Articles in the Same Issue
Aims and Scope of Reformulation
Lloyd, J., Ryle, A., Hepple, J. and Nehmad, A., 2011. Aims and Scope of Reformulation. Reformulation, Winter, p.64.
Black and White Thinking: Using CAT to think about Race in the Therapeutic Space
Brown, H. and Msebele, N., 2011. Black and White Thinking: Using CAT to think about Race in the Therapeutic Space. Reformulation, Winter, pp.58-62.
Book Review: "Why love matters – How affection shapes the baby’s brain" by Sue Gerhardt
Poggioli, M., 2011. Book Review: "Why love matters – How affection shapes the baby’s brain" by Sue Gerhardt. Reformulation, Winter, p.43.
CAT, Metaphor and Pictures
Turner, J., 2011. CAT, Metaphor and Pictures. Reformulation, Winter, pp.39-43.
Comment on James Turner’s article on Verbal and Pictorial Metaphor in CAT
Hughes, R., 2011. Comment on James Turner’s article on Verbal and Pictorial Metaphor in CAT. Reformulation, Winter, pp.24-25.
Compassion in CAT
Wilde McCormick, E., 2011. Compassion in CAT. Reformulation, Winter, pp.32-38.
Equality, Inequality and Reciprocal Roles
Toye, J., 2011. Equality, Inequality and Reciprocal Roles. Reformulation, Winter, pp.44-48.
Letter from the Chair of ACAT
Hepple, J., 2011. Letter from the Chair of ACAT. Reformulation, Winter, p.4.
Letter from the Editors
Lloyd, J., Ryle, A., Hepple, J. and Nehmad, A., 2011. Letter from the Editors. Reformulation, Winter, p.3.
Supervision Requirements across the Organisation
Jevon, M., 2011. Supervision Requirements across the Organisation. Reformulation, Winter, pp.62-63.
The Chicken and the Egg
Hepple, J., 2011. The Chicken and the Egg. Reformulation, Winter, p.19.
The Launch of a new Special Interest Group
Jenaway, Dr A., Sachar, A. and Mangwana, S., 2011. The Launch of a new Special Interest Group. Reformulation, Winter, p.57.
The PSQ Italian Standardisation
Fiorani, C. and Poggioli, M., 2011. The PSQ Italian Standardisation. Reformulation, Winter, pp.49-52.
The Reformulation '16 plus one' Interview
Yabsley, S., 2011. The Reformulation '16 plus one' Interview. Reformulation, Winter, p.67.
Using Cognitive Analytic Therapy for Medically Unexplained Symptoms – some theory and initial outcomes
Jenaway, Dr A., 2011. Using Cognitive Analytic Therapy for Medically Unexplained Symptoms – some theory and initial outcomes. Reformulation, Winter, pp.53-55.
What are the important ingredients of a CAT goodbye letter?
Turpin, C., Adu-White, D., Barnes, P., Chalmers-Woods, R., Delisser, C., Dudley, J. and Mesbahi, M., 2011. What are the important ingredients of a CAT goodbye letter?. Reformulation, Winter, pp.30-31.
Whose Reformulation is it Anyway?
Jenaway, Dr A., 2011. Whose Reformulation is it Anyway?. Reformulation, Winter, pp.26-29.
Working within the Zone of Proximal Development: Reflections of a developing CAT practitioner in learning disabilities
Frain, H., 2011. Working within the Zone of Proximal Development: Reflections of a developing CAT practitioner in learning disabilities. Reformulation, Winter, pp.6-9.
"They have behaviour, we have relationships?"
Greenhill, B., 2011. "They have behaviour, we have relationships?". Reformulation, Winter, pp.10-15.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.