The Chicken and the Egg
Hepple, J., 2011. The Chicken and the Egg. Reformulation, Winter, p.19.
Question: How do you find out which comes first, the chicken or the egg?
Answer: Go to a restaurant and ask the waiter for a chicken and an egg, and see which comes first.
Unfortunately, the waiter is likely to ask you: ‘Do you want the egg with the chicken or as a starter / dessert?’ This engagement in dialogue makes every outcome possible, corrupts any predictive method and results in the answer to the chicken and egg question being: ‘It depends’ or ‘On this occasion the egg came before the chicken, but in another context it could be the other way round, or at the same time (chicken omelette!)’.
Welcome to the indeterminate world of dialogism!
Transference and Counter-transference
The subject of transference and counter-transference (enactment) is a complex and a confusing area. I think it can be made easier at the start by acknowledging that perhaps the whole idea is simply a metaphor to describe something of the process by which human beings engage with each other, particularly in the therapy setting. One of the confusions comes with attempts to objectify and reduce the phenomenon to, using a deceptively simple metaphor, a game of tennis where someone serves up the ball (projection perhaps in analytic terms) and someone then receives it and returns it. This looks like something that can be captured and modelled – or does it?
The reality of a dialogic exchange between two human beings is indeterminate and unfinalisable. Any ‘shot’ is aimed by a particular player at another particular player taking into account the anticipated strengths and limitations of each. Also, and perhaps most importantly for the theme of this paper, the game is only ever observed in play. There is no serve and no winning shot. As Bakhtin writes: ‘There is neither a first word or a last word. The contexts of dialogue are without limit. They extend into the deepest past and the most distant future. Even meanings born in dialogues of the remotest past will never be finally grasped once and for all, for they will always be renewed in later dialogue’. (Bakhtin, 1986).
For example, a client’s expectations of you as a therapist may be coloured by stories of her grandmother’s experience of psychoanalysis in the 1940s. As a therapist you have picked up on something in the tone of the referral letter long before you have had any experience of this particular client directly. This has resonated with a prejudice about ‘this sort of client’ from your previous experience. The enactment has started long before the first session and your experience of this therapy will colour your future encounters with people you meet in your life, including future clients.
Let us have a quick look now at the beginnings of this amazing idea; that the relationship between client and therapist is a rich source of understanding for the therapeutic process. One of the first mentions of transference by Freud is:
‘…the patient is frightened at finding that she is transferring on to the figure of the physician the distressing ideas which arise from the content of the analysis.’ (Freud, 1895).
And then:
‘…a whole series of psychological experiences are revived, not as belonging to the past, but as applying to the person of the physician at that particular moment….others are more ingeniously constructed….by cleverly taking advantage of some real peculiarity in the physician’s person or circumstances and attaching themselves to that.’ (Freud, 1905).
Freud’s first use of ‘counter transference’:
‘We have become aware of the ‘counter-transference’, which arises in him as a result of the patient’s influence on his unconscious feelings, and we are almost inclined to insist that he shall recognise this counter-transference in himself and overcome it…’ (Freud, 1910).
This seems to suggest that the client begins the process by perceiving in the therapist (with some concession, in 1905, that not all therapists are the same) some similarity with a relational experience from her past and experiencing the thoughts, feelings and behaviours associated with that previous relationship in the context of the current relationship with the therapist. It is worth noting that fifteen years passed before counter-transference emerged as an idea that could be brought into the therapy thinking. Initially seen as an obstacle or ‘resistance’ to therapy, Freud developed the idea that the transference relationship, and its analysis, was an important driving force behind therapeutic change.
There have been many additions to the conceptualisation of the transference relationship in the psychoanalytic situation since Freud, including the ideas of ‘positive’ and ‘negative’ transference, ‘transference neurosis’, ‘transference psychosis’, ‘erotized transference’, ‘transference-cure’, and ‘delusional transference’ (Sandler et al 1973, Chapters 4 and 5). These make interesting reading, but it is here that most of us get lost in complexity and real conceptual difficulty in laying each concept alongside or on top of another in a way that makes logical sense. Perhaps we are trying too hard to theorize something which is really just a metaphor for a human, dialogic exchange that cannot be finalized or reduced in this way.
Voloshinov (one of the ‘Bakhtin School’) wrote an important critique of the analytic stance in the 1920s:
‘In the whole Freudian construct of a psychical conflict, together with all the mechanisms through which it operates, we hear only the biased voice of the subjective consciousness (the therapist) interpreting human behaviour. The unconscious is nothing but one of the motives of that consciousness, one of its devices for interpreting behaviour ideologically….Freud’s theory is a ‘projection’ of certain object relations of the external world into the world of the psyche. What finds expression there is the extremely complex social relationship between doctor and patient….
Not a single instance of verbal utterance can be reckoned exclusively to its utterer’s account. Every utterance is the product of the interaction between speakers and the product of the broader context of the whole complex social situation in which the utterances emerge’.
(Voloshinov. In: Morris (ed.), 1994).
This critique draws attention to the ‘chronotype’; the two particular persons in the room and the wider context of their encounter in time and space involving all the complexities of social, cultural and historical influences affecting both the back-story of the individuals and the back-story of the setting itself; the analytic situation. Ryle and Kerr (2002) draw attention to the power differential of the analytic situation:
‘The conventional analytic reciprocal role pattern locates power in the analyst and could be summarised (or perhaps caricatured) as:
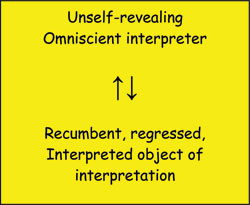
(Ryle and Kerr, 2002)
Ryle (1982) acknowledges that the opacity of the analyst is a deliberate strategy to evoke dependency and the uncovering of primitive and infantile material, but he argues that:
“…for many patients, the inaccessibility and remoteness feels hostile and may mirror their own inability to stay in touch with others. Such patients may struggle through to the recognition that the analyst is offering care but, in my view, the way to this recognition need not in most cases be made so hard”. (Ryle, 1982)
Ryle and Kerr state CAT’s position:
‘Therapist and patient roles are not symmetrical but they are of equal value and the aim should be to base them on openness and mutual respect’. (Ryle and Kerr, 2002.)
Ryle also makes it clear that there is nothing unique about encounters in the therapy relationship:
‘Patient-Therapist relationships are one example of a more general model of relationships’. (Ryle, 1998).
He also reminds us that the formation of a therapy relationship based on ‘genuine human commitment to the patient’ provides a ‘unique opportunity for change’:
‘One skill of the therapist, therefore, is to allow his patients to use the relationship as a stage on which to play out versions of his scripts, especially those felt as unacceptable or not fully known. Another therapist’s skill is to recognise and use fully those small-scale interactions that take place on the therapeutic stage to illustrate higher-order scripts which are responsible for the patient’s life difficulties’. (Ryle, 1982)
This clearly puts the therapy relationship and the opportunity that enactments offer at the heart of a CAT therapy, but does this give us enough to work on when deciding how to use interchange between client and therapist in the therapy relationship to encourage reflection and change? This is perhaps the most important task for the CAT therapist, given that repair of therapy enactments that threaten therapy rupture is linked to positive therapy outcome (Daly et al, 2010).
Ryle and Kerr go further by describing subdivisions of counter-transference, which have become pretty well established in CAT theory:
‘A person enacting one pole of a reciprocal role procedure may either:
Convey the feelings associated with the role to others, in whom corresponding empathic feelings may be elicited or
Seek to elicit the reciprocating response of the other.’ (Ryle and Kerr, 2002.)
In another discussion of reciprocating counter-transference Ryle uses a well know CAT adage:
‘The therapist’s job here is simple – not to join the dance’. (Ryle, 1998.)
By this I think he is sensibly warning about the dangers of reciprocating rejecting or critical role play in an unreflected-upon way. As I will expand on later, I would suggest that when the therapist becomes aware of the enactment they are already dancing, or at least tapping their feet to the music, and it is the choice of what to do next; how to use the enactment, that determines whether the dance leads to rupture or repair. CAT has always been strong on using the counter-transference therapeutically. As I heard Tony Ryle say at a CAT South workshop:
‘How the client makes you feel in the session is (usually) the client’s business’.
There is one further subdivision of counter-transference in psychoanalysis that has been borrowed by CAT theory; that elicited by the client and that personal to the back-story of the therapist:
‘Elicited counter-transference will be a response to whatever role the patient is playing and is therefore ‘news’ about the patient. It may coincide with but needs to be clearly differentiated from the therapist’s personal counter-transference derived from his or her own array of procedures.’ (Ryle, 1998).
Although this is a helpful reminder that particular therapists may have strong and unhelpful responses to particular clients and that good supervision is essential to practice of CAT, I wonder if we have gone down a road of too many overlapping sub-categories that in an attempt to simplify end up muddying the water; as the real experience of a therapist in enactment with a client will not easily separate out into personal/elicited, empathic/reciprocating components.
I suggest that the CAT concept of reciprocal roles, and the possibility of describing an enactment in the therapy relationship using reciprocal role mapping, is big enough to allow integration of these sub-categories and parallel perspectives in a way that can simplify and aid reflection in supervision and help the therapist use knowledge of enactment therapeutically with the client.
In summary I suggest that the concept of reciprocal role enactment in CAT allows integration in four areas:
- Integration of the separation of the therapy setting from other encounters between people. Reciprocal role enactment in the therapy relationship is one example of a general description of human relating, in a particular boundaried setting. Consideration of the whole context of the therapy setting (particularly the power inequalities) is crucial to a real dialogue, but this again cannot be easily generalised; each setting/client/therapist will have its own unique character and nuances. The negotiated boundaries, therapeutic alliance and the skill of the therapist, however, do allow a frank discussion of the nature of this relationship that can lead to therapeutic change and self-reflection.
- Integration of the analytic concepts of transference (client experience of therapist) and counter-transference (therapist response to client) into a reciprocal role relationship that does not have a clear beginning or end (enactment).
- Integration of the ‘personal’ and ‘elicited’ components of the enactment in the therapist. The boundaries of the therapy relationship and the use of supervision can allow acceptance that what is ‘going down’ in the room is inevitably to do with the whole person of the client and the whole person of the therapist. My response to a client is my response to a client. It is to do with my own experience and back-story – a client may be trying to elicit a particular response in me according to their own back-story expectations but this may or may not work with me, and I am different from therapist x, y or z. What results is a unique encounter that can be mapped and brought into dialogue with therapeutic benefit.
-
Integration of ‘top’ and ‘bottom’ role polarisation. This is more controversial but it may be possible to hold on to the idea that (as I heard Tony explain at the same workshop): ‘Reciprocal Roles are a necessary simplification, and are a wonderful starting point for bringing enactment into dialogue, but that Reciprocal Roles are only a metaphor or sign for a more complex dialogic encounter that is ‘shimmering’ around the room (to borrow a ‘Potterism’).
In the example below I have tried to map out how the client and therapist can be experiencing both ‘top’ and ‘bottom’ role feelings, thoughts and behaviours at the same time.
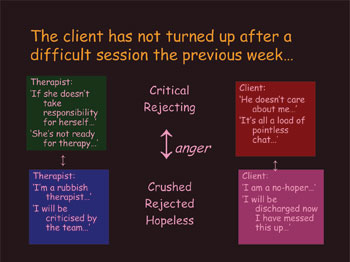
In order to ‘slow down’ an enactment and bring it into dialogue the therapist may need to be open to the whole range of ways that they may be experiencing the client/therapist relationship. This includes the whole context of the setting, the back-stories of the client and therapist and an openness to the fact that they may be experiencing uncomfortable ‘bottom’ roles and retaliatory ‘top’ roles at the same time. This seems a big ask but is, I think, what we already try to do in supervision. In order to use enactment therapeutically we need to be open to it in all its frightening and confusing manifestations.
Enactment, in this description, is a dialogic concept and so cannot be finalized or fully pinned down. In each encounter in the therapy setting the roots of the enactment stretch back in time to involve voices and influences from the distant past (both personal to the therapist and client and more general to the control and solid context of the setting). The encounter, as mapped by a Reciprocal Role or procedure, is simply a glimpse of the ‘ball in play’; as soon as it is captured in some way it moves on, transforms and draws in more responses. This is the richness that we can draw on in the work we do with clients.
To summarise, it seems to me that therapeutic use of enactment involves:
- Establishing a trusting and respectful relationship that ‘gives permission’ for clients to play out their ‘scripts’ in a safe and boundaried setting.
- The therapist being open to all the thoughts, feelings and behaviours they are experiencing in the context of enactment.
- Avoidance of potentially unrepairable ruptures.
- The establishment of an ‘alongside’ or observing (eye) position where both client and therapist can use their curiosity about the enactment as a rich source of material for dialogue.
- The therapist using self-reflection and supervision to make considered choices as to how to use awareness of enactment therapeutically in a meaning-making dialogue with the client.
A final word on the ‘microcosm’ of enactment. In the course of helping therapists work with particular enactments with clients in supervision or in workshops, I have been struck by the depth of understanding that can be achieved by trying to trace back the enactment to its roots in the therapy relationship; ‘when did you first notice something was going on?’. This awareness may take the form of a ‘voice’ in the therapist that expresses an honest feeling about the client. It may be a strong feeling or sensation or may take a more metaphorical form in a dream or waking imagery that seems to sum up a moment in time.
An experience like this, once allowed to unravel, often holds within it much information about deeply felt and often disavowed experiences from the client’s past, often to do with early neglect, abandonment and abuse that can be overlooked in a therapy that has focussed on a battle for control or the maintenance of mutual admiration between client and therapist.
The word ‘microcosm’ is derived from the Greek words ‘mikros’ and ‘cosmos’; literally ‘little world’. It holds the idea that even the smallest part contains something of a representation of the whole; the universe in a raindrop; the first chicken as a tiny black speck inside the first chicken’s egg?
Post-script
According to evolutionists the first bird’s egg must have been laid by a reptile, from which birds are thought to have evolved. The first bird’s egg, in this sense came before the first bird and it was laid by a reptile but had the potential to grow into a bird due to mutation. But hang on…..the mutation must have happened to the fertilised cluster of cells before the egg was formed around them…..it seems unlikely, however, that the first bird was a chicken. Perhaps we’ll leave it there; unfinalized as usual!
References
Bakhtin,M. M (1986) Speech Genres and other late essays. (trans. V.W. Maghee, eds. C. Emerson and M. Holquist). Austin, Texas: University of Texas Press.
Bakhtin, M. M (1990) Author and hero is aesthetic activity. In M M Bakhtin, Art and answerability: Early philosophical works by M. M. Bakhtin, eds. M Holquist and V Liapunov, trans. V Liapunov. Austin Texas: Texas University Press.
Daly, A-M, Llewellyn, S and McDougall, E (2010). Rupture resolution in the cognitive analytic therapy for adolescents with borderline personality disorder. Psychology and Psychotherapy: Theory, Research and Practice. 83, 273-288.
Freud, S (1895) Studies on hysteria. Standard Edition, 2, London: Hogarth Press.
Freud, S (1905) Fragment of an analysis of a case of hysteria. Standard Edition, 7, London: Hogarth Press.
Freud, S (1910) Letter to Ferenczi of 6 October. 1910, quoted in Jones, E
Sigmund Freud his life and works, Vol. 2, New York: Basic Books, 1955.
Morris, P (ed.) (1994) The Bakhtin Reader: Selected writings of Bakhtin, Medvedev, Voloshinov. London: Arnold.
Ryle, A (1982 ) Transference: the metaphoric relationship between patient and therapist. In: A. Ryle, Psychotherapy - A Cognitive Integration of Theory and Practice, Academic Press, 1982.
Ryle, A (1994) Projective identification; a particular form of reciprocal role procedure. British Journal of Medical Psychology 67: 107-114.
Ryle, A (1998) Transference and Countertransferences: the Cognitive Analytic Therapy perspective. British Journal of Psychotherapy 14 : 303–309.
Ryle, A (2001) CAT’s dialogic perspective on the self. ACAT News 15: 3-4.
Ryle, A and Kerr, I B (2002) – Introducing Cognitive Analytic Therapy. Principles and Practice. Chichester: Jon Wiley & Sons
Sandler, J Dare, C and Holder, A (1973) The patient and the analyst. London: Karmac Books.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Hepple, J., 2011. The Chicken and the Egg. Reformulation, Winter, p.19.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Relationships in Microcosm in Cognitive Analytic Therapy: Based on a workshop given at the 2012 ACAT Conference in Manchester
Hepple, J., 2012. Relationships in Microcosm in Cognitive Analytic Therapy: Based on a workshop given at the 2012 ACAT Conference in Manchester. Reformulation, Winter, pp.35-38.
A Little Bit Of Bakhtin - From Inside To Outside And Back Again
Hepple, J., 2010. A Little Bit Of Bakhtin - From Inside To Outside And Back Again. Reformulation, Winter, pp.17-18.
Developing a Language for the Psychotherapy of Later Life
Hepple, J., 2006. Developing a Language for the Psychotherapy of Later Life. Reformulation, Winter, pp.23-28.
Psycho-Social Checklist
-, 2004. Psycho-Social Checklist. Reformulation, Autumn, p.28.
The Experience Of The Psychiatric Interview Following Self-Harm
Nevison, C., 2000. The Experience Of The Psychiatric Interview Following Self-Harm. Reformulation, ACAT News Spring, p.x.
Other Articles in the Same Issue
Aims and Scope of Reformulation
Lloyd, J., Ryle, A., Hepple, J. and Nehmad, A., 2011. Aims and Scope of Reformulation. Reformulation, Winter, p.64.
Black and White Thinking: Using CAT to think about Race in the Therapeutic Space
Brown, H. and Msebele, N., 2011. Black and White Thinking: Using CAT to think about Race in the Therapeutic Space. Reformulation, Winter, pp.58-62.
Book Review: "Why love matters – How affection shapes the baby’s brain" by Sue Gerhardt
Poggioli, M., 2011. Book Review: "Why love matters – How affection shapes the baby’s brain" by Sue Gerhardt. Reformulation, Winter, p.43.
CAT, Metaphor and Pictures
Turner, J., 2011. CAT, Metaphor and Pictures. Reformulation, Winter, pp.39-43.
Comment on James Turner’s article on Verbal and Pictorial Metaphor in CAT
Hughes, R., 2011. Comment on James Turner’s article on Verbal and Pictorial Metaphor in CAT. Reformulation, Winter, pp.24-25.
Compassion in CAT
Wilde McCormick, E., 2011. Compassion in CAT. Reformulation, Winter, pp.32-38.
Equality, Inequality and Reciprocal Roles
Toye, J., 2011. Equality, Inequality and Reciprocal Roles. Reformulation, Winter, pp.44-48.
Letter from the Chair of ACAT
Hepple, J., 2011. Letter from the Chair of ACAT. Reformulation, Winter, p.4.
Letter from the Editors
Lloyd, J., Ryle, A., Hepple, J. and Nehmad, A., 2011. Letter from the Editors. Reformulation, Winter, p.3.
Supervision Requirements across the Organisation
Jevon, M., 2011. Supervision Requirements across the Organisation. Reformulation, Winter, pp.62-63.
The Chicken and the Egg
Hepple, J., 2011. The Chicken and the Egg. Reformulation, Winter, p.19.
The Launch of a new Special Interest Group
Jenaway, Dr A., Sachar, A. and Mangwana, S., 2011. The Launch of a new Special Interest Group. Reformulation, Winter, p.57.
The PSQ Italian Standardisation
Fiorani, C. and Poggioli, M., 2011. The PSQ Italian Standardisation. Reformulation, Winter, pp.49-52.
The Reformulation '16 plus one' Interview
Yabsley, S., 2011. The Reformulation '16 plus one' Interview. Reformulation, Winter, p.67.
Using Cognitive Analytic Therapy for Medically Unexplained Symptoms – some theory and initial outcomes
Jenaway, Dr A., 2011. Using Cognitive Analytic Therapy for Medically Unexplained Symptoms – some theory and initial outcomes. Reformulation, Winter, pp.53-55.
What are the important ingredients of a CAT goodbye letter?
Turpin, C., Adu-White, D., Barnes, P., Chalmers-Woods, R., Delisser, C., Dudley, J. and Mesbahi, M., 2011. What are the important ingredients of a CAT goodbye letter?. Reformulation, Winter, pp.30-31.
Whose Reformulation is it Anyway?
Jenaway, Dr A., 2011. Whose Reformulation is it Anyway?. Reformulation, Winter, pp.26-29.
Working within the Zone of Proximal Development: Reflections of a developing CAT practitioner in learning disabilities
Frain, H., 2011. Working within the Zone of Proximal Development: Reflections of a developing CAT practitioner in learning disabilities. Reformulation, Winter, pp.6-9.
"They have behaviour, we have relationships?"
Greenhill, B., 2011. "They have behaviour, we have relationships?". Reformulation, Winter, pp.10-15.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.