K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples
Jenaway, A., 2009. K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples. Reformulation, Winter, pp.13-16.
Having worked for the last five years with adolescents using CAT, and trying to modify it to make it more adolescent friendly, I wanted to share my thoughts. My hope is that others who are also working with this group of patients will write in to Reformulation with their experiences. I have really tried to simplify the letters and diagrams that I use with adolescents. I hope that these attempts at simplification, without losing the vital elements of CAT, might also be helpful to those working with difficult to engage patients of any age.
Are Adolescents so Different?
Adolescents are probably similar to any patients that are difficult to engage. However, they do have the double whammy of a developmental lack of self-reflection as well as that caused by any difficult experiences they have had so far. Also, adolescents are in general, much more interested in the day-to-day details of their life than in their past, or the general direction in which they are heading. They generally come into therapy wanting help with a specific problem, such as self-harm, r. Rather than wanting to understand their whole personality and the underlying procedures leading to the problem. We may be able to see that living a life without making any plans does not bode well for the future, but they are just going with the flow and can’t always see the bigger picture. We may be able to see that having been abused, and then rejected, by their mother has left them angry and mistrustful, but they do not want their mother to even be discussed as she is a waste of space and they never cared about her anyway!
- Self-reflection is often very poorly developed. Although the literature suggests that it should be coming on board by around 4 years of age, and developing rapidly from then, it seems to be very delayed in adolescents who have had difficult early experiences. Facing up to the reality of a situation that you do not have any power to change can be aversive, so again, it feels better to focus on the day to day.
- For teenagers, transient relationships have immense importance, so a boyfriend of one week deserves the same kind of reverence as a partner of ten years. Suggesting otherwise requires tact and diplomacy in the therapist.
- Adolescents have little power socially, and few resources to influence the social system around them. They may well be dependent on parents to get them to sessions, and to fund any possible activities that you come up with as exits to their procedures. Encouraging them to be more assertive with their parents may well be counterproductive and cause more conflict. It is also important to remember that most of their social interactions are with other adolescents, not the most reasonable, mature, tolerant individuals with whom to practice newly learned reciprocal roles.
- There is inevitably a huge power imbalance between therapist and patient. The therapist is seen very much as an authority figure, like a parent or teacher, in real life terms as well as in the transference. One teenager I worked with repeatedly referred to the “last lesson” rather than the “last session”.
In general the literature on psychotherapy with adolescents emphasises that focussing on engagement should be given greater importance than getting a good history (or reformulation) or insisting on following a particular model of therapy. At first, CAT seems to fit very well with this idea, but, in fact, we do rely quite a bit on people telling us about their past experiences and relationships. I remember coming to a screeching halt in my mind the first time an adolescent refused to tell me anything about his past because it would make him get really angry and he might hit me. How could I ever get a reformulation out of that? Of course, if you keep it simple, the reformulation is already there in the dilemma:
Either completely out of touch with feelings or overwhelmed and furiously angry
But I didn’t know then that that could be enough to start with.
Engaging Adolescents in CAT
The most important thing that I have discovered is to follow their agenda rather than insisting on the “CAT agenda”. If they want to talk about the film they saw last night then let them, listen to their response to it and find the reciprocal roles. Use their heroes, their favourite stories, their favourite song, film, TV programme as much as possible. I have found myself taking on a therapeutic role with a lighter touch, more humourus, less “deep and meaningful”. Responding to, and validating difficult feelings but not pushing them to stay there, if they need to move on and talk about something lighter. Letting them dip in and out of the difficult stuff at their own pace. Even so I have had several dropouts who have said, “Iit’s too painful to talk about this stuff”. Tony Ryle’s take on engagement was that people become engaged when the process starts to make sense for them and they can see that it could be helpful. I try to capture a key dilemma as early as possible and start to draw that in a diagram – using their images or getting them to draw it if I can. The dilemma above might be drawn as either a locked cupboard or an explosion, with the task of therapy being to find the middle ground, where feelings could be felt, thought about and contained without exploding. There is plenty of time to add the reciprocal roles in words later if you need to.
These diagrams, which may include only a single dilemma, or a single trap, are much more manageable for adolescents to take on board. As before, they are not really interested in their whole personality, just the problem they came with. Focussing on this problem straight away helps with engagement, and can be done even if they do not want to talk about the past. The image I have is of trying to feed a wild bird. You would not offer a banquet of rich food that would be confusing and overwhelming. You would offer a small titbit of something simple and easy to digest, if they take it, and start to trust you, then you can give them something richer. I do try to work towards a reformulation letter with most adolescents but I tend to do this alongside using the simple diagram and talking about the “exit” of the middle ground and how they are doing with finding that. The letter can take a bit longer than four sessions.
Modifying the Tools
I do not use the psychotherapy file with adolescents as I think it is too complex for many of them. I have modified one of the tools of schema focused cognitive therapy, which is a list of statements about the self in simple terms, e.g. “I give more to people than I get back in return”. It is easier to explain, and I think, easier to fill in. The procedures in CAT terms are very easy to relate to the groups of statements but, again, it starts off simple and can be built up later on. I have added a few positive statements such as “I am a good listener” -- which most people with placation are -- so that the person is not ticking a relentless list of negative things about themselves. As described above, I try to keep the diagrams as simple as possible. Usually they include just a dilemma with two positions – the place I am trying to get away from and the extreme place I go to which is not successful either. The work is inevitably about finding the middle ground, what that would look like, who they know who is in the middle, where I seem to be as a therapist etc.
The reformulation letter can also be a bit relentlessly negative if the person has had a very difficult time. I tend to write less about the awful things they did have and more about the important things they didn’t have. For example, “… it is so sad that you did not have anyone to talk to about what was happening to you, to reassure you and encourage you to keep going.” This can lead smoothly on to what they might need to do to improve things.
I do not use conventional rating sheets, as these do not seem very popular. I think they feel a bit too much like homework. I tend to use a solution-focused way of rating. If the middle ground is 10 out of 10, and you were at 0 when we met, then where are you now?” This seems to work well and can still provide a regular rating of progress.
Finding Aims and Exits and Being a Good Parent to Yourself
This seems to come naturally from the letter and the diagram. If the middle place is where you need to be, then you need to stop doing so much of the extremes and imagine the middle. I introduce the idea of reciprocal roles at this point (if I have not already described them in the letter). I describe how, as teenagers, we have to take on the role of “parenting ourselves” as we become independent. Unfortunately, we tend to parent ourselves the way we have been parented, unless we think about it and choose to do something different. The middle ground is a place where you are being a better parent to yourself. Any reactions or behaviour can then be considered in the context of whether it showed that they were being a good parent to themselves or not. This tends to make it feel less criticism and more like sadness when they have done something risky or unhelpful. In a way it means that the aim and exits are rather vague and abstract, but it seems to work better than pinning them down to a verbal description, which never seems to capture all the aspects of being a good parent! It also provides a useful way to discuss the parental transference in the therapeutic relationship, “although I can never be your real parent, I can show you what it feels like to be listened to in these sessions”.
Another advantage of working on the intrapersonal self-parenting is that it is in many ways a safer option than working on the interpersonal self to other roles. Encouraging young people to express their feelings to another, for example, can lead to more upset and rejection if they are expressing them to a parent who cannot validate or comfort. Often, there is someone in the family or nearby who is supportive, but not always. Learning to really listen to your own feelings and take them seriously, and learning to comfort yourself, is often a safer and more reliable option.
Adolescents are often reluctant to do anything different in a deliberate way. They will be adamant that it won’t work, they’ve tried it already, it would be too embarrassing etc. However, they often tell me at a later session that they have done just what I suggested. I am rarely given credit for the advice though, it usually “just happened” or was suggested by someone at school/church/a friend. I have come to see that the unconscious, internalisation of new reciprocal roles can be a much more powerful, and rapid, process with adolescents than with older adults. They can rapidly start to value themselves more, feel that they are worth standing up for and behave accordingly. Obviously this is not always the case, but it does make me want to champion early intervention for personality problems.
Case Example
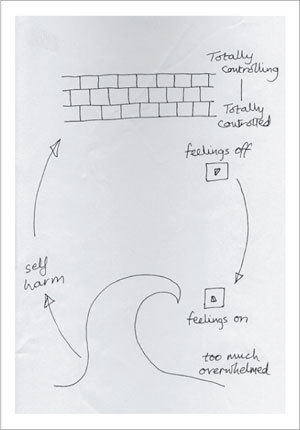
Adam was a fifteen year old who was suffering from depression and had been self harming. He had been sent home from boarding school because they could not cope with him there. His relationship with his parents sounded reasonable, they had split up when he was nine years old and he had lived with his mother, to whom he was closer. He described his father as a bit controlling, a perfectionist. He had been badly bullied at boarding school but had never told either parent. On returning home, he had had a few sessions of cognitive behaviour therapy but did not like it and dropped out so CAT was suggested. He was tall and slim and dressed as a Goth, all in black and with black eye makeup. He said that he had wanted to dress that way for a while but had only recently had the courage to do so. He had also recently come out as gay and started a relationship with a boyfriend. He didn’t know why he wanted to dress like a Goth – it just appealed to him. Putting other people off wasn’t a problem as the people that got to know him would be the ones who had really made the effort. He showed very little non-verbal communication and was strange to interact with. He said that he put a lot of effort into reading other’s body language to predict what they were thinking, but he made sure that he did not show any feelings and did not give anything away. In the waiting area, before the first session, he was drawing in a sketch book. I showed an interest in looking at his art, wondering what the drawings might reveal, but he proudly told me that the drawings would look identical whatever mood he was in. He described putting up a dam so that others couldn’t see his feelings and I drew a wall at the top of the diagram (see SDR). This felt safer for him, as he was in control, but was strange for others. We came to see that he was also using the dam to block out any difficult feelings and this meant that he was switching off feelings and was out of touch with them. He did not see this as a problem as he thought that his feelings were irrelevant and that others would not be interested in them, they would just be a nuisance. The problem was that sometimes feelings broke through the dam and they were like a tidal wave. That was when he self harmed – somehow that got the dam back in place. We added the tidal wave and, later the feelings switch which was either off (at the top of the diagram) or on (at the bottom). We talked at length about the pros and cons of this and whether it might be better to have a “feelingsometer” rather than merely a switch. That way he might know then what he was feeling more of the time and detect it earlier when feelings were building up. Having never let his feelings through, he had not learned how to cope with them in healthier ways, he wasn’t getting any practice. Thus the middle ground might be “being more aware of feelings, learning to comfort myself, risking expressing them sometimes”. Adam did not like my description of this middle ground as being a better parent to himself, but he could see that this might be a better place to be than the two extremes which he ended up in. He decided, at first, to experiment with letting others see how he felt by allowing some non-verbal body language to show. He discovered that people around him started to ask what was wrong and gave him the opportunity to talk about things before they got to the tidal wave stage. He started to see that expressing feelings was sometimes useful and gradually stopped feeling the need to self harm. Other work led to him feeling better about himself but the key change seemed to be the “feelingsometer”.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Jenaway, A., 2009. K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples. Reformulation, Winter, pp.13-16.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Book Review: Self-Harm Assessment in Young People – A Therapeutic Assessment manual By Dennis Ougrin, Tobias Zundel and Audrey V. Ng Published by Hodder Arnold, 2010
Jenaway, Dr A., 2010. Book Review: Self-Harm Assessment in Young People – A Therapeutic Assessment manual By Dennis Ougrin, Tobias Zundel and Audrey V. Ng Published by Hodder Arnold, 2010. Reformulation, Summer, p.49.
What Happens After “Happy Ever After�
Jenaway, A., 2010. What Happens After “Happy Ever After�. Reformulation, Summer, pp.8-9.
Letter to the Editors
Janet Toye, 2013. Letter to the Editors. Reformulation, Winter, p.4.
Change your Parenting for the Better - exploring CAT as a parenting intervention
Dr Alison Jenaway, 2013. Change your Parenting for the Better - exploring CAT as a parenting intervention. Reformulation, Winter, p.32,33,34,35,36.
Thoughts and Experiences of the Application of Cognitive Analytic Therapy to Clinical Work with Adolescents
Mulhall, J., 2010. Thoughts and Experiences of the Application of Cognitive Analytic Therapy to Clinical Work with Adolescents. Reformulation, Summer, pp.34-36.
Other Articles in the Same Issue
A Brief Survey of Perceptions of Cognitive Analytic Therapy Within Local Mental Health Systems
Turley, A., Faulkner, J., Tunbridge, V., Regan, C. and Knight, E., 2009. A Brief Survey of Perceptions of Cognitive Analytic Therapy Within Local Mental Health Systems. Reformulation, Winter, p.26.
A Call For Papers On The 3rd International ACAT Conference
Elia, I., 2009. A Call For Papers On The 3rd International ACAT Conference. Reformulation, Winter, p.25.
A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities
Wells, S., 2009. A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities. Reformulation, Winter, pp.21-23.
Chair’s Letter, October 2009
Westacott, M., 2009. Chair’s Letter, October 2009. Reformulation, Winter, p.3.
Cognitive Analytic Therapy, or Can You Make a Mad Man Sane?
Anonymous, 2009. Cognitive Analytic Therapy, or Can You Make a Mad Man Sane?. Reformulation, Winter, pp.11-13.
Darwin and Psychotherapy
Elia, I., 2009. Darwin and Psychotherapy. Reformulation, Winter, p.9.
Dialogue and Desire: Michael Bakhtin and the Linguistic Turn in Psychotherapy by Rachel Pollard
Hepple, J., 2009. Dialogue and Desire: Michael Bakhtin and the Linguistic Turn in Psychotherapy by Rachel Pollard. Reformulation, Winter, pp.10-11.
International ACAT Conference “What Constitutes a CAT Group Experience?â€
Anderson, N., M., 2009. International ACAT Conference “What Constitutes a CAT Group Experience?â€. Reformulation, Winter, pp.25-26.
IRRAPT 2007-9 Research Projects
McNeill, R., 2009. IRRAPT 2007-9 Research Projects. Reformulation, Winter, p.26.
K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples
Jenaway, A., 2009. K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples. Reformulation, Winter, pp.13-16.
Letter from the Editors
Elia, I., Jenaway, A., 2009. Letter from the Editors. Reformulation, Winter, p.3.
Letter to the Editors
Anonymous, 2009. Letter to the Editors. Reformulation, Winter, p.6.
Measurements of change and their relationship to each other in the course of a CAT therapy
Gallagher, G., Inge, T., McNeill, R., Pretorius, W., O’ Rourke, D. and Wrench, M., 2009. Measurements of change and their relationship to each other in the course of a CAT therapy. Reformulation, Winter, pp.27-28.
Recieving a CAT Reformulation Letter: What Makes a Good Experience?
Newell, A., Garrihy, A., Morgan, K., Raymond, C., and Gamble, H., 2009. Recieving a CAT Reformulation Letter: What Makes a Good Experience?. Reformulation, Winter, p.29.
Research Into the Use of CAT Rating Sheets
Coombes, J., Taylor, K. and Tristram, E., 2009. Research Into the Use of CAT Rating Sheets. Reformulation, Winter, pp.28-29.
The Big Debate - Health Professions Council
Jenaway, A., 2009. The Big Debate - Health Professions Council. Reformulation, Winter, p.7.
Threats to Clinical Psychology from the CBT Stranglehold
Lloyd, J., 2009. Threats to Clinical Psychology from the CBT Stranglehold. Reformulation, Winter, pp.8-9.
Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.
When Happy is not the Only Feeling: Implications for Accessing Psychological Therapy
Lloyd, J., 2009. When Happy is not the Only Feeling: Implications for Accessing Psychological Therapy. Reformulation, Winter, pp.24-25.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.