Helping service users understand and manage the risk: Are we part of the problem?
Crowther, S., 2014. Helping service users understand and manage the risk: Are we part of the problem?. Reformulation, Winter, pp.41-44.
There is now an impressive evidence base that Cognitive Analytic Therapy can be adapted and used by people with Learning Disabilities (LD) and those that support them (Lloyd & Clayton, 2013). Key to this body of work is how people with LD, their staff teams/carers and the wider system can get caught up in unhelpful and damaging reciprocal role procedures (RRPs). In my work in a forensic service for people with LD, I have been interested in how the very nature of forensic systems and the dominant ways of thinking in such settings can re-enact unhelpful, but common RRPs for people with LD. In this brief article I want to provide some examples of this and show how CAT can be used to work with these challenges.
Reciprocal Roles in Forensic Settings
It has been suggested that people with LD possess a narrower range of reciprocal roles due to the limited range of relationships they are exposed to (Lloyd & Williams, 2003). For people who present with harmful behaviour the opportunities for different types of relationships are often limited and even further limited by the focus of others on their problematic behaviour and potential risk. Due to the damaging impact of this behaviour, its eradication becomes the main focus. Others often take a critical and punishing stance, communicating to the person that their behaviour is unacceptable and needs to stop, but the underlying function of the behaviour is missed. Therefore, the way in which secure settings understand and respond to risk behaviour is very important; if we are not careful we can unwittingly re-enact the very behaviours that we are trying to support service users to reduce.
The following two case formulations provide examples of this. The formulations are based on my clinical experiences, but some of the detail and personalisation has been removed so as to provide a thematic representation that draws out the key issues. In both cases the function of the risk behaviour appears to relate to ‘control’, and for staff working in this setting this aspect is easily recognised as they may refer to such service users as ‘controlling’ or ‘needy’, but the function of control in the emotional life of the individual is often then overlooked.
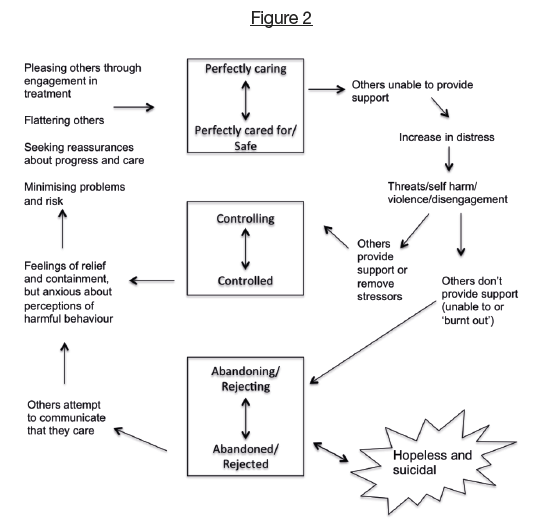
Figure 1: Feeling Safer when others are there for me.
Service users who are anxious about being rejected and abandoned can seek safety and containment through a ‘perfectly caring-perfectly cared for’ RRP. This could be conceptualised as an ‘idealised’ place, but it is also precarious. Ultimately the RRP can’t last because others are unable to live up to the service user’s expectations. As the service user starts to fall from this RRP, their level of anxiety increases and they become overwhelmed. Risk behaviour in the form of self-harm, threatening behaviour and violence is then an attempt to elicit a controlling-controlled RRP. This can be self to self, to reduce overwhelming emotions; self to others, to gain extra support from others; or others to self, to invite others to take control. If others are not able to respond to this heightened anxiety, perhaps due to the competing needs of other service users, or if they, themselves, are overwhelmed (i.e. frustrated, angry, despairing, etc.) this enacts a rejecting/abandoning-rejected/abandoned RRP. This RRP represents a ‘dreaded place’ and prolonged periods of time here are likely to lead to suicidal behaviour, due to the isolation and hopelessness experienced at these times. This RRP is also expressed self to self, as service users feel low in mood and start to self-neglect (refusing food, medication, showers, etc.) and self to other, as they often also disengage from attempts to help them. Service users often move from this ‘dreaded place’ following prolonged efforts from the staff team to communicate that they care about the service user. In my experience, this is when staff members are more likely to find themselves blurring boundaries by doing things such as hugging service users, revealing personal information, making promises and spending long periods of time with the service user to the exclusion of others, in order to try and help the person out of this RRP.
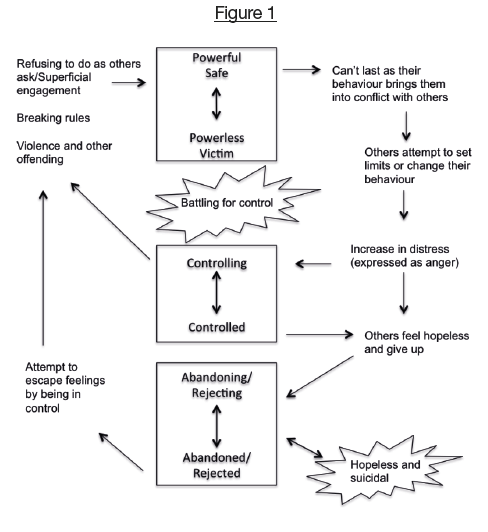
Figure 2: Feeling safer when others are kept away from me
For other individuals, safety is sought through keeping others at a distance. For such service users the ‘idealised place’ can be conceptualised as a ‘powerful/in charge- powerless/victim’. Often they have experienced rejection and abuse from others, which has been associated with a belief that they are worthless and bad. This leads to a strong mistrust of others, which is managed by trying to remain in the ‘powerful/in charge’ RRP at all costs. However, it is not possible to remain in this idealised place as their behaviour brings them into conflict with others by committing offences or breaking rules. Services in the form of the Police, the Courts and secure settings attempt to place limits and control their behaviour, whilst service users continue to resist this. Their behaviour escalates until they are detained and therefore ‘controlled’ by others. When they arrive in a forensic setting, service users continue to try to get to the idealised place through attempts to remain in control (self to self and self to other). This may take the form of refusing to engage with others, challenging any perceived threat, or engaging but on a superficial level.
However, what then develops are repetitive cycles of battling for control between service users and staff members/services.
This can lead to high levels of frustration and hopelessness in the staff team, leading them to ‘give up’ and reject/abandon the service user in the form of moving them to a different ward, hospital or a higher level of security. For service users this abandoning/rejecting response of others can connect them to painful feelings of being rejected and blamed. Such feelings are often rarely accessed because they are associated with vulnerability. Service users are therefore at a greater risk of self-harm and suicide at these times due to the connection to these painful feelings. Rather than be in touch with these feelings service users may try to feel in control again in whichever way possible, for example by making threats to others or by refusing medication, thus continuing the battle for control.
Therefore, in secure settings there is nearly always an invitation into a controlling-controlled RRP, and unless this is formulated and understood by staff, it can prevent the development of more adaptive behaviours and perpetuate risk behaviours. Conversely, it is also possible to see how a ‘controlling-‘compliant/pleasing’ enactment could enable service users to give the impression that they are making progress without developing adaptive alternatives to risk behaviours.
Difficulties Exploring Risk
The discussion of risk with service users can be fraught with difficulties as individuals use different strategies that discourage exploration, from continuous ‘I don’t know’ responses to hostile and threatening behaviour. For some individuals simply acknowledging that they need help is exposing and stigmatising. Wilberforce describes how accepting help from others can be seen to reflect unwanted associations with vulnerability, impairment and a sense of dependency: “an interaction can only be perceived as ‘caring’ or helpful, if the recipient perceives themselves as in need of such help or care and if not it may be more like interference or even oppression” ( Wilberforce, 2013,p. 113). For people with LD a sense of being different from others has often been experienced throughout life, thus a sense of needing care and support can be associated with shame, and thus is strongly defended against; despite the offer of help being well meaning.
A further complicating factor in the exploration of risk is that this aspect of the self is not always immediately and easily accessible. Individuals who are at greater risk of harming others have often experienced trauma, abuse and neglect (Pollock & Stowell-Smith, 2006). Such experiences give rise to polarised and restricted reciprocal role repertoires and disassociated self-states (Ryle and Kerr, 2002). Thus, an individual’s ability to reflect and explore feelings is likely to be compromised, and they are unlikely to have a full understanding of their harmful patterns (Shannon, 2009). For people with LD this ability to reflect, explore and describe their internal states is compromised further by their intellectual ability (Clayton, 2013).
The consequence of these difficulties is that staff members and service users reciprocally collude in avoiding the issue of discussing risk. This increases the likelihood of falling back into the ‘controlling-controlled’ RRP, as service users focus on ‘staying out of trouble’ and ‘complying with treatment’, leaving staff members believing that progress is being made based on service users’ willingness to comply.
Therefore, in helping people with LD develop greater insight into their risk potential, I often feel stuck between the service structures that seem to enact unhelpful RRPs and the service users own difficulties in exploring their risk. Progress is only likely to be achieved if we can support people to explore the risk they pose to others, in a collaborative manner, tailored to their zone of proximal development (Vygotsky, 1978), in a way that seeks to avoid feelings of shame and judgement.
Mapping Out Contextual Enactments
Potter (2013) refers to helping as a ‘dance’, which highlights the importance of noticing and naming the ‘dance’ that services and service users are caught up in. Thus, as a starting point I have found it helpful to use the reformulation tools to map out the familiar patterns around control in therapy sessions with service users, staff teams and multidisciplinary teams. Having this ‘on the table’ provides some distance from an often emotionally demanding experience and allows all to stand back and consider how those involved in the system may be enacting particular aspects of an RRP. This then leads to a consideration about the best way forward and promotes a collaborative approach, which aims to empower service users to have a voice about the help they are offered.
Using SDRs To Increase Understanding And Compassion
Harmful behaviour often leaves members of staff feeling confused, hurt and overwhelmed. These feelings can create barriers to the development of relationships, and this is reflected at the times when service users complain that staff members ‘don’t understand’ and ‘don’t care’. Using the reformulation tools, I have been able to reconceptualise harmful behaviours as a Target Problem Procedures that comprise aims, beliefs, behaviours and consequences. This can help staff members empathise with the difficulties service users have in eliciting care and managing feelings, which then allows staff members to consider alternative responses that do not enact unhelpful procedures.
Using Validation When Talking About Risk
For both parties, talking about risk can be an uncomfortable process with service users often minimising the harm they cause others or attempting to change the conversation to avoid the issue being discussed. These interactions are an enactment in the relationship that needs to be reflected upon. A discussion about this often reveals that the service user was feeling anxious about discussing risk and apprehensive about the reaction of others. Naming how difficult it is to talk about risk is often validating and enables a move to mapping out what happens when risk is not discussed. Drawing this out helps service users to recognise that avoidance perpetuates the behaviour, as they do not gain greater insight into the thoughts and feelings that motivate their risk behaviour.
Conclusion
In my experience, working in a secure setting with people with LD can invite ‘doing to’, rather than ‘doing with’ reciprocal role procedures due to concerns about risk. This is problematic in terms of service user empowerment and involvement, and also on a broader level, if people with LD are only offered the same relationships and dialogue, which perpetuate the same risk- laden identities, change is unlikely to occur and risk behaviour is likely to continue. Whilst this is a complex issue, I believe that CAT is ideally placed to meet some of these challenges through contextual reformulations and service user empowerment.
References
Clayton, P. (2013). The adaption and adoption of tools in Cognitive Analytic Therapy for people who have an intellectual disability and their carers. In Lloyd, J. & Clayton, P. (Eds.) Cognitive Analytic Therapy for people with Intellectual Disabilities and their carers (pp. 42-53). Jessica Kingsley.
Lloyd, J. & Clayton, P. (Eds.) (2013). Cognitive Analytic Therapy for people with Intellectual Disabilities and their carers. Jessica Kingsley.
Lloyd, J. & Williams, B. (2003). Reciprocal Roles and the ‘unspeakable known’: exploring CAT within services for people with intellectual disabilities. Reformulation, Summer, 19-25.
Pollock. P.H., Stowell-Smith, M. (2006). Cognitive Analytic Therapy applied to offending. In Pollock. P.H., Stowell-Smith. M. & Gopfert M. (Eds.). Cognitive Analytic Therapy for Offenders: A New Approach to Forensic Psychotherapy. (pp. 1-42). Routledge.
Potter, S. (2013). The helper’s dance list. In: Lloyd, J. & Clayton, P. (Eds.) Cognitive Analytic Therapy for people with Intellectual Disabilities and their carers (pp. 89-96). Jessica Kingsley.
Ryle, A. and Kerr, I. B. (2002). Introducing Cognitive Analytic Therapy. Principles and Practice. Wiley: Chichester
Shannon, K. (2009). Using what we know : cognitive analytic therapy’s contribution to risk assessment and management. Reformulation, Winter, 16-21.
Vygotsky, L. S. (1978). Mind in society. Cambridge, MA: Harvard University Press.
Wilberforce, D. (2013). The problems of caring and being cared for (or how to get your shoelaces tied for you). In: Lloyd & Clayton (Eds.) Cognitive Analytic Therapy for people with Intellectual Disabilities and their carers (pp. 109-121). Jessica Kingsley.
Simon is a Clinical Psychologist and CAT practitioner in training, working in a secure setting with adults with Learning Disabilities for Calderstones Partnership NHS Foundation Trust
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Crowther, S., 2014. Helping service users understand and manage the risk: Are we part of the problem?. Reformulation, Winter, pp.41-44.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
The 4P’s model: A Cognitive Analytic Therapy (CAT) derived tool to assist individuals and staff groups in their everyday clinical practice with people with complex presentations
Phyllis Annesley and Lindsay Jones, 2016. The 4P’s model: A Cognitive Analytic Therapy (CAT) derived tool to assist individuals and staff groups in their everyday clinical practice with people with complex presentations. Reformulation, Summer, pp.40-43.
How CAT-Informed Practice Can Help To Improve Mental Health Services
Ben Bell, 2017. How CAT-Informed Practice Can Help To Improve Mental Health Services. Reformulation, Winter, pp.33-37.
BOOK REVIEW: Cognitive Analytic Therapy for people with intellectual disabilities and their carers
Lloyd, J,. and Clayton, P., 2014. BOOK REVIEW: Cognitive Analytic Therapy for people with intellectual disabilities and their carers. Reformulation, Summer, pp.10-11.
Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services
Fisher, C., Harding, C., 2009. Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services. Reformulation, Summer, pp.4-5.
Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.
Other Articles in the Same Issue
A Dog in the World of ACAT
Gray, M, 2014. A Dog in the World of ACAT. Reformulation, Winter, pp.11-14.
A New Concept of Understanding CAT and Hermeneutics
Bobvos-Bekefi, M., 2014. A New Concept of Understanding CAT and Hermeneutics. Reformulation, Winter, pp.22-32.
Bringing Bodies Into Dialogue
Dower, C., 2014. Bringing Bodies Into Dialogue. Reformulation, Winter, pp.15-21.
CAT and CFT - Complementary in the treatment of shame?
Jameson, P., 2014. CAT and CFT - Complementary in the treatment of shame?. Reformulation, Winter, pp.37-40.
Dear Homeland: CAT At The Edinburgh Festival
Kirkland, J. Potter, S. Affleck, D., 2014. Dear Homeland: CAT At The Edinburgh Festival. Reformulation, Winter, pp.9-10.
Editorial
LLoyd, J. Pollard, R., 2014. Editorial. Reformulation, Winter, pp.2-3.
Helping service users understand and manage the risk: Are we part of the problem?
Crowther, S., 2014. Helping service users understand and manage the risk: Are we part of the problem?. Reformulation, Winter, pp.41-44.
Letter from the Chair of ACAT
Hepple, J, 2014. Letter from the Chair of ACAT. Reformulation, Winter, pp.4-5.
Politics, Reciprocal Roles and Dialogue
Welch, L., 2014. Politics, Reciprocal Roles and Dialogue. Reformulation, Winter, pp.6-8.
Words and Rituals: The significance of 'smaller' endings
Sher, M., 2014. Words and Rituals: The significance of 'smaller' endings. Reformulation, Winter, pp.33-36.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.