Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services
Fisher, C., Harding, C., 2009. Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services. Reformulation, Summer, pp.4-5.
This paper comes from discussion between a CAT supervisor (CF) who works in adult mental health and a clinical psychologist colleague (CH) working in Learning Disability Services (LD).
We have written this as an exploratory paper to share our thoughts and would very much welcome comments and additions to the ideas we discuss here.
Learning Disability and Challenging Behaviour
Many referrals in Learning Disability services are requests to respond to people with behaviours that challenge. This includes a range of behaviours such as physical aggression, verbal aggression, damage to property and self harm. The most widely used definition of behaviours that challenge is:
“culturally abnormal behaviour(s) of such intensity, frequency or duration that the physical safety of the person or others is placed in serious jeopardy, or behaviour which is likely to seriously limit or deny access to the use of ordinary community facilities”.
(Emerson, 1995)
In essence, such referrals are usually considered with the principle of understanding the antecedents (triggers), behaviours and consequences surrounding the behaviour that challenges, and using this information to guide the staff team to build up proactive ways of reducing problematic behaviours while promoting positive alternatives.
This approach relies upon the assumption that behaviours have an identifiable trigger (usually thought of as external) to which individuals are responding. This is often an effective way of understanding and managing behaviours that challenge. For example, a client who finds noisy environments very anxiety provoking may be more likely to self harm when the person they live with has their extended family to visit.
Within this approach lies an assumption that the behaviours that challenge services are actually unhelpful ways of someone attempting to meet their needs. This understanding sounds very like the CAT concept of a problem procedure.
As well as viewing this as a problem procedure, a CAT perspective invites us to consider that it is likely that the ‘challenging behaviour’ will be linked to a Reciprocal Role (RR) for that client. Holding the CAT perspective further, pushes us to consider the possibility that the responses to such behaviours (e.g. from staff or other clients) may well fit in with the client’s RRs opening up the possibility that we may inadvertently be reinforcing the very behaviour we are aiming to prevent.
There is a growing literature that describes using CAT in indirect work. This has included ideas about psychologically harmful environments (Walsh, 1996) and Contextual Reformulation (Ryle and Kerr, 2002). It is suggested here that the systems in which we work are themselves full of Reciprocal Roles within which individual people (whether clients or staff) fit more or less easily. In large organisations, such as the NHS, this may often be multi-layered, with sets of RRs being enacted within and between different groups such as clients, staff teams and senior staff teams (e.g. Bancroft et al, 2008). CAT would suggest that these RRs are likely to be most problematic when they are enacted unknowingly and it is, therefore, most useful to reflect on the sorts of RRs that might be common to all levels of the wider system. Such an example is the ‘rebel’ role.
The ‘Rebel Role’
Diagram 1: Reciprocal Role including the Rebel Role
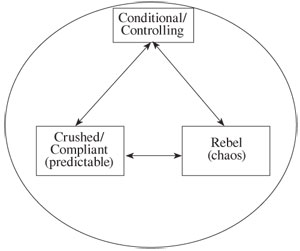
The Reciprocal Role, described in diagram 1 is commonly seen in life and in work with clients. An example from adult mental health might be of a client describing issues of high expectations, control and compliance in childhood and presenting with an eating disorder in which the roles may be currently enacted self to self. ‘Conditional/controlling’ might equate to imposing dietary restraint; ‘crushed/compliant’ to anorexic behaviour and ‘rebel’ to bulimic behaviour. I’ve tended to have a general rule of thumb about this reciprocal role that taking the ‘rebel’ role is generally the more healthy option (as in normal adolescent behaviour) and is more likely to lead to exits although this can, of course, be taken to an unhelpful extreme.
We realised that this RR is commonly seen in clients with LD and in the systems that surround them. Control is (perhaps necessarily) imposed on a client (for example about how independently they live). Everything is stable as long as the client remains compliant and the controlling system is stable and unchallenged. However, if the client moves across to the rebel role, pushing against the boundaries and control imposed by the system, then a reaction of imposing further controls is often triggered. Further ‘rebellion’, may perhaps be labelled ‘challenging behaviour’.
In one common pattern, the system becomes increasingly controlling in an attempt to achieve greater predictability and avoid the chaos of ‘rebel’ behaviour. This can, in the end, lead to further rebellion/chaos or to situations in which the client complies, but in which the level of control imposed on them may underestimate their real capability. In one example we came across, a discussion that started about staff concerns for the safety of a client who was becoming increasingly independent quickly progressed to the idea of imposing a 7pm curfew.
This illustrates how the enactment of this RR can tend to limit advances in the client’s independence and control. A client making such an advance may be seen as attempting to take control, thus leaving staff feeling either crushed or threatened and rebellious. In neither case, is the client likely to be appropriately supported. Clearly, this is more likely to occur if these RR patterns resonate with the system’s reciprocal roles.
‘Challenging behaviour’ often leads to referral to the clinical psychologist. If we consider the possibility that the challenging behaviour may represent the ‘rebel role’ as on diagram 1, then it can be seen that the psychologist is often called in with the explicit aim of moving the client back to the ‘compliant’ role. This seems to fit uneasily with the idea that the rebel role (within limits) is often the more healthy option. It also seems to place the psychologist in the uncomfortable position in which their intervention is either aimed to restrict and limit the client by supporting imposed controls or, if the psychologist challenges the RRs in operation, they themselves are likely to be seen as rebellious and generally unhelpful to the system.
Exits
So what might an exit look like from this problematic reciprocal role that seems to be widespread both in individuals and systems? We have found the following formulation helpful.
Diagram 2: The Exit
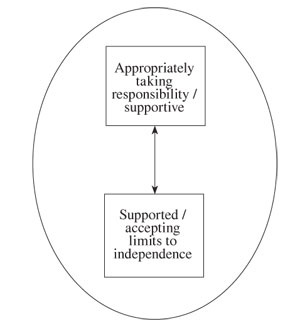
If we consider this first at the level of an individual client in relation to a care system, this exit suggests that needs will be fully considered and that appropriate levels of independence will be supported. It also implies that passivity (as in the ‘crushed’ role above) is no longer completely desirable: in this RR, everyone in the system needs to consider taking an appropriate level of responsibility.
The exit also has something to say about the way many systems adopt the RR in diagram 1. It is understandable that a system will prefer predictability to chaos and that this can reinforce the system imposing controls that have a tendency to crush (We imagine anyone working in the NHS can think of examples!). A true challenge both to staff and management teams would be to find ways to facilitate everyone in the system taking appropriate responsibility and accepting the limits of their independence within a mutually supportive environment.
Finally
Clearly we are not suggesting that this provides an understanding of all challenging behaviour or that this will be helpful in work with all individuals.
The exit described here of taking appropriate responsibility and accepting limits of independence fits with the stated service philosophy within LD of empowerment for service users. It may also be helpful for the therapist to reflect upon how a referral may invite them into a ‘controlling’ or a ‘rebel’ role and how they can help themselves and staff teams, as well as clients, move towards an exit role.
References
Bancroft, A, Collins, S, Crowley, V, Harding, C, Kim, Y, Lloyd, J and Murphy, N. 2008. Is CAT an island or a Solar System? The dilemmas in the therapeutic frame when working with people in learning disabilities services. Reformulation 30. Summer 2008.
Emerson, E. 1995. Challenging behaviour: analysis and intervention with people with learning difficulties. Cambridge: Cambridge University Press
Ryle, A and Kerr, I B. 2002.Introducing Cognitive Analytic Therapy: Principles and Practice. Chichester: John Wiley & Sons.
Walsh, S. 1996. Adapting cognitive analytic therapy to make sense of psychologically harmful environments. British Journal of Medical Psychology.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Fisher, C., Harding, C., 2009. Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services. Reformulation, Summer, pp.4-5.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Helping service users understand and manage the risk: Are we part of the problem?
Crowther, S., 2014. Helping service users understand and manage the risk: Are we part of the problem?. Reformulation, Winter, pp.41-44.
Creatively Adapting CAT: Two Case Studies from a Community Learning Disability Team
Smith, H., Wills, S., 2010. Creatively Adapting CAT: Two Case Studies from a Community Learning Disability Team. Reformulation, Winter, pp.35-40.
Reciprocal Roles and the 'Unspeakable Known': Exploring CAT within Services for People with Learning Disabilities
Lloyd, J. and Williams, B., 2003. Reciprocal Roles and the 'Unspeakable Known': Exploring CAT within Services for People with Learning Disabilities. Reformulation, Summer, pp.19-25.
Is CAT an Island or Solar System?
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.
Reflecting on my first placement - A CAT understanding to illustrate learning
Louise Johnson, 2013. Reflecting on my first placement - A CAT understanding to illustrate learning. Reformulation, Winter, p.9.
Other Articles in the Same Issue
A Little Italian Story – Service Development
Fiorani, C., Poggioli, M., 2009. A Little Italian Story – Service Development. Reformulation, Summer, pp.13-14.
Aims and Exits from Self-Defeating Procedures
Toye, J., 2009. Aims and Exits from Self-Defeating Procedures. Reformulation, Summer, pp.26-29.
Book Review of: Beatrice Beebe and Frank Lachmann (2002). Infant Research and Adult Treatment: Co-constructing Interactions. Published London: Analytic Press.
Lloyd, J., 2009. Book Review of: Beatrice Beebe and Frank Lachmann (2002). Infant Research and Adult Treatment: Co-constructing Interactions. Published London: Analytic Press.. Reformulation, Summer, pp.34-35.
Book Review of: How Infants Know Minds. Reddy, V. (2008). Harvard University Press.
Ryle, T., 2009. Book Review of: How Infants Know Minds. Reddy, V. (2008). Harvard University Press.. Reformulation, Summer, pp.33-34.
CAT and People with Learning Disability: Using CAT with a 17 Year Old Girl with Learning Disability
David, C., 2009. CAT and People with Learning Disability: Using CAT with a 17 Year Old Girl with Learning Disability. Reformulation, Summer, pp.21-25.
CAT Effectiveness: A Summary
Quraishi, M., 2009. CAT Effectiveness: A Summary. Reformulation, Summer, pp.36-38.
Letter from the Editors
Elia, I., Jenaway, A., 2009. Letter from the Editors. Reformulation, Summer, p.3.
Meeting with Older People as CAT Practitioners: Attending to Neglect
Sutton, L., Gaskell, A., 2009. Meeting with Older People as CAT Practitioners: Attending to Neglect. Reformulation, Summer, pp.6-13.
Obtaining Consent to Publish – Further Thoughts
Toye, J., Lloyd, J., Jenaway, A., 2009. Obtaining Consent to Publish – Further Thoughts. Reformulation, Summer, p.3.
Reflections on Our Experience of Running a Brief 10-Week Cognitive Analytic Therapy Group
John, Dr C., Darongkamas, J., 2009. Reflections on Our Experience of Running a Brief 10-Week Cognitive Analytic Therapy Group. Reformulation, Summer, pp.15-19.
State Regulation of Psychotherapy: Protecting the Public or ‘Professionalising’ Psychotherapy at the Expense of Therapeutic Integrity, Creativity and Diversity?
Pollard, R., 2009. State Regulation of Psychotherapy: Protecting the Public or ‘Professionalising’ Psychotherapy at the Expense of Therapeutic Integrity, Creativity and Diversity?. Reformulation, Summer, pp.29-31.
The CAT Articles Review
Knight, A., 2009. The CAT Articles Review. Reformulation, Summer, p.32.
Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services
Fisher, C., Harding, C., 2009. Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services. Reformulation, Summer, pp.4-5.
Update on Statutory Regulation
Westacott, M., 2009. Update on Statutory Regulation. Reformulation, Summer, p.20.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.