Is CAT an Island or Solar System?
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.
In this write up of a discussion that took place in the Learning Disability Special Interest Group on October 2007, we look at the role conflicts we are pulled into in terms of traps, dilemmas and snags and explore what roles we are working towards.
Our discussion comes from the CAT therapist’s perspective, but we also wonder what it is like as a CAT supervisor or a client receiving therapy.
What is CAT for those working in learning disability services?
As for many experienced professionals, because CAT integrates and then develops on earlier theories, we find in CAT an image of the predominant frameworks operating in our service and from our training. For us, CAT resonates with our behavioural and systemic frameworks. What are Reciprocal Roles if not mutual stimulus and response? Just as for those coming from a predominantly object relations background, the concept of RR encapsulates fundamental ideas from their original theory, so for those of us from behavioural backgrounds, there is a comfortable sense of being at home with CAT. For example, whereas in behavioural terms we refer to ABCs (Antecedent, Behaviour and Consequence), in CAT we find a similar account in one of the procedural sequences described as a trap. CAT’s relational model is suited to the systemic nature of learning disability work in which our working context involves negotiating and collaborating with multiple agencies. We find in CAT an inherently elegant approach that respects all the therapeutic models we encounter, so we can easily swap lexicons whilst retaining the same meanings i.e., this is the dialogic nature of CAT.
However, learning disability work is not where CAT originated. We experience discomfort and dissonance at times, created by the CAT emphasis on its models of origin. We wonder whether these frames of origin have become working habits that get confused with CAT? This is particularly so for those approaches which see the therapeutic boundary as a sealed container. In working with people with Learning Disabilities, working systemically is essential in the treatment effort. Given this, we are then bound to ask, what are the ethics of our work within staff teams and systems?
The roles we are pulled into
In thinking about the ethics, a starting point could be thinking about our roles. In LD services, one of the most common roles is the rescuing RR. Another one is the narcissistic position of the therapist as we are an elitist profession, particularly priding ourselves on working in highly complex systems with highly complex people. We also have a fantasy of a CAT THERAPIST, which involves where we think the client ought to be. Maybe we are being over-optimistic towards therapists and clients, if we imagine there is a neat 16-session therapy after which the client’s life changes permanently for the better. We may find ourselves on both the receiving and initiating ends of this ideal, when we and our supervisor demand this as the minimal benchmark for therapeutic success. Furthermore, NHS managers and members of the multi-disciplinary team, the staff team and the client’s family often make similar demands. In complex cases, however, which describe the vast majority of our work, it is not like this. CAT is about looking at what is blocking our client from moving on. CAT helping the client to move on is different from expecting removal of all problems.
Traps
Seeing others as making demands and not as others who can offer us support, we therapists try to be supportive but experience endless demands. The trap is that we strive to meet everyone’s needs except our own. Then we end up feeling exhausted, depleted and useless.
When we think of Reciprocal Role Procedures to do with striving and perfection, so common among CAT practitioners who wish to heal, how do we find they influence our attempts not to become a parental authority, but to remain collaborative in therapy?
Are boundaries in learning disability work a brick wall or a permeable membrane?
Our clients may not be aware of the pull of the other aspects of the therapist’s world. They may not know how their therapist is embedded within and indeed licensed by and commissioned to practice by wider systems. Similarly, we often forget how our client may experience being pulled by other clients who also know us, in our roles within day centres and residential homes. Those other clients may know us in roles different from a CAT therapist, such as our main roles in being their psychologist or nurse. Are there common roles for CAT therapists and clinical psychologists or nurses, or are these roles inevitably exclusive?
Furthermore, it is up to our clients whether or not they maintain the confidentiality we seek to offer them. Examples which come to mind include the client putting her Sequential Diagrammatic Reformulation [SDR] on the fridge in her residential home for all to see, or a client requesting that a copy of the Reformulation be placed in their file. We know how helpful it can be when clients choose to produce their diagram and explain it to others, as CAT tools can help them find their voice. At other times, however, a therapeutic aim might be to help the client learn that they have a right to confidentiality, privacy and boundaries, especially when they have little experience of this. We need to discuss collaboratively with each client the pros and cons of where both the therapist’s and the client’s work might best lie on a continuum of confidentiality and working together.
Given the collaborative stance of CAT, how are staff, carers and families viewed? Are the staff, carers and families the deliberate cause of the client’s problems, or unwittingly colluding with RRPs that they have not had an opportunity to think about or discuss? Are these people trying to manage very difficult and complex situations as best they can? Are they experts on the client, and can they help us learn what works best with them? Are the staff, carers, and family the client’s best, most frequent and extended opportunity to experience what new, helpful and productive RRPs feel like? Do we struggle against their influence, ignore them, separate from them, try to educate them, or do we prefer CAT’s collaborative, respectful stance where we seek to discuss how to work together, including exploring what boundaries might be helpful?
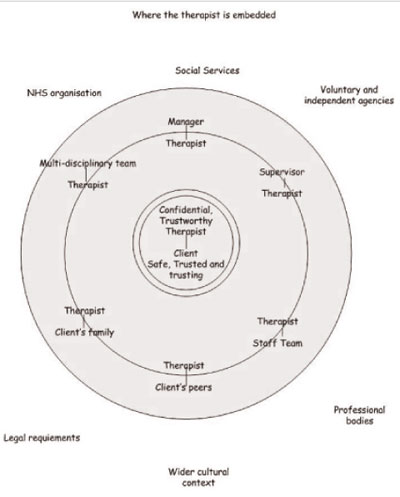
This diagram attempts to describe the system both we and our clients find ourselves in.
Dilemma
The dilemma may be described as whether CAT is an island or whether it is a part of a solar system.
We wish therapy to be safe and contained. There is a fantasy that it is possible to conduct therapy totally removed and separated from the world, as a complete unit ‘entire unto itself’, with no breach of confidentiality. It would feel easier to be able to stay in a safe, confidential place. This is an ideal therapeutic environment, but we have the dilemma of the demands of the wider system and our main dilemma is around our accountability to this wider system. For example, some of us have had our process notes (which, in the NHS, are the property of the Secretary of State for Health, not ours) subpoenaed by the Court.
Either CAT with tough boundaries excludes a care co-ordinating role, or CAT coincides with our core professions and involves care co-ordination. But is this care consultation or co-ordination role necessary? If it were considered to be, then how could we carry both the role of therapist and of care consultant or co-ordinator?
Confidentiality is a fantasy from the perspective of working in multi-disciplinary teams where we must attend meetings and be involved in risk management processes such as Care Programming Approaches and Safeguarding Vulnerable Adults meetings. We seek to deal with this tension by discussing with our clients what they want in regard to their therapist attending such meetings. This may be different from what the system wants, and so we have a dilemma that needs to be negotiated. There may also be a difference between the client’s goal and the therapist’s goal. If the client is not contained, we may have to relate to the professional system, acting in our client’s best interest, which may damage the relationship with the client. CAT is about clear and accurate description about what goes on for the client, but in relating to the wider system, could the information we offer be used against the client?
Most of our clients with learning disabilities have to have co-operation from the team because their own control over their lives is reduced and they require enhanced learning opportunities in order to be able to recognise and revise unhelpful RRPs. This creates a dilemma around either focusing on individual work with the client or focusing on work with the team and all the demands from the wider system including family or criminal courts and the police. Sometimes this can be resolved by being able to divide these tasks amongst professionals, but sometimes community health teams lack the resources to be able to involve several professionals.
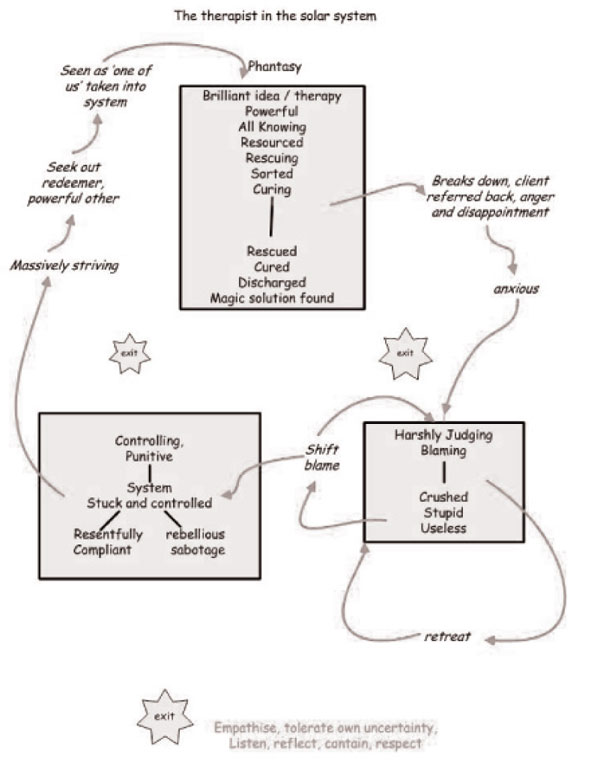
One result of this dilemma is that we experience not being understood, not just by other workers but also sometimes by supervisors who are not experienced in or do not accept that working in community teams means being aware of real-world relationships and complexities. The result is we become more fragile than we would like to be. This happens when we are put in a pivotal role in relation to our client’s needs, the needs of the service and of wider society. Demands are placed on us as if we are the centre of the whole system. The SDR below that we developed at our January meeting describes what this situation can be like - See Diagram Overleaf.
Positive Reciprocal Roles and Procedures
If the client could perform some of the therapist’s ‘relating to the team’ duties, such as when the client rather than the therapist tells the team about their diagram, then power belongs to the client within their orbit. We hope that this can lead to the client’s support group continuing to meet to explore and discuss ways of helping the client according to CAT suggestions but without needing the CAT therapist’s direct input.
What are the roles that we need to strive to maintain? Most of all we would like a respecting – respected role. This is especially challenging for us in our attitudes towards support workers and families as it is so easy for us to slip into a blaming – blamed role. We would also like to be in a good enough role rather than endlessly striving. We think it is useful to ask ourselves, are we rescuing or are we providing a supportive space?
How can we think about the tension of these dilemmas? We need our observing eye. Is there a strong rationale for the therapeutic and other roles of a CAT therapist working with LD clients being rigorously separated? Our answer to this for our complex cases is often ‘no’. All the relational thinking we use to formulate, work systemically, supportively and contextually with and case manage our clients cannot be separated from a therapeutic role. The main issue for us is how to work with the relational space/matrix in which the client’s mental health is held, maintained and or damaged. In an ideal world we would build a healthy boundary around the therapy. However, the relational space of the LD client and their therapy is partly internal, i.e., woven into their personality, and partly social i.e., woven into the surrounding organisational, social, and cultural context that makes up the client’s life space. A psychotherapist or CAT practitioner needs to be able to work across these areas, and confidentiality and boundaries need to be negotiated within these relational dynamics.
We would like to thank Annie Nehmad and Barbara Williams for their helpful comments about this paper.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services
Fisher, C., Harding, C., 2009. Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services. Reformulation, Summer, pp.4-5.
Trauma, Trauma and More Trauma: CAT and Trauma in Learning Disability
Julie Lloyd, 2019. Trauma, Trauma and More Trauma: CAT and Trauma in Learning Disability. Reformulation, Summer, pp.44-46.
Relational patterns amongst staff in an NHS Community Team
Staunton, G. Lloyd, J. Potter, S., 2015. Relational patterns amongst staff in an NHS Community Team. Reformulation, Summer, pp.38-44.
Confidentiality and Good Record Keeping in CAT Therapy - A Discussion Paper
Brown, H., 2010. Confidentiality and Good Record Keeping in CAT Therapy - A Discussion Paper. Reformulation, Summer, pp.10-12.
Creatively Adapting CAT: Two Case Studies from a Community Learning Disability Team
Smith, H., Wills, S., 2010. Creatively Adapting CAT: Two Case Studies from a Community Learning Disability Team. Reformulation, Winter, pp.35-40.
Other Articles in the Same Issue
CAT Used Therapeutically and Contextually
Murphy, N., 2008. CAT Used Therapeutically and Contextually. Reformulation, Summer, pp.26-30.
Catch up with CAT
Potter, S., Curran, A., 2008. Catch up with CAT. Reformulation, Summer, p.54.
Clinical Implications for the Pregnant CAT Therapist
Knight, A., 2008. Clinical Implications for the Pregnant CAT Therapist. Reformulation, Summer, pp.38-41.
Consent to Publish in Reformulation
Jenaway, A., Lloyd, J., 2008. Consent to Publish in Reformulation. Reformulation, Summer, p.7.
Cuckoo Lane
Selix, M., 2008. Cuckoo Lane. Reformulation, Summer, p.6.
How to Enjoy Writing a Prose Reformulation
Wilde McCormick, E., 2008. How to Enjoy Writing a Prose Reformulation. Reformulation, Summer, pp.16-17.
Integration of Cognitive Analytic Therapy Understandings
Ruppert, M., Birchnall, Z., Bruton, C., Christianson, S., 2008. Integration of Cognitive Analytic Therapy Understandings. Reformulation, Summer, pp.20-22.
Is CAT an Island or Solar System?
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.
Letter from the Chair of ACAT
Westacott, M., 2008. Letter from the Chair of ACAT. Reformulation, Summer, pp.3-4.
Letter from the Editors
Elia, I., Jenaway, A., 2008. Letter from the Editors. Reformulation, Summer, p.3.
Metaprocedures in Normal Development and in Therapy
Hayward, M., McCurrie, C., 2008. Metaprocedures in Normal Development and in Therapy. Reformulation, Summer, pp.42-45.
Plugging in and Letting Go: the Use of Art in CAT
Hughes, R., 2008. Plugging in and Letting Go: the Use of Art in CAT. Reformulation, Summer, pp.9-10.
Service Innovation
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.
Silence in Practice
Harvey, L., 2008. Silence in Practice. Reformulation, Summer, pp.11-13.
The ‘Human Givens’ Fast Trauma and Phobia Cure
Jenaway, A., 2008. The ‘Human Givens’ Fast Trauma and Phobia Cure. Reformulation, Summer, pp.14-15.
The Body in Dialogue
Burns-Lundgren, E., Walker, M., 2008. The Body in Dialogue. Reformulation, Summer, pp.18-19.
The Development of the Sequential Diagrammatic Reformulation
Parkinson, R., 2008. The Development of the Sequential Diagrammatic Reformulation. Reformulation, Summer, pp.33-37.
The States Description Procedure
Hubbuck, J., 2008. The States Description Procedure. Reformulation, Summer, pp.46-53.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.