Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice
Wicksteed, Dr. A., 2012. Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice. Reformulation, Summer, pp.26-31.
Evidence Base and Theoretical Rationale for Using CAT to treat Eating Disorders
The evidence base for using CAT in working with people with eating disorders remains small at this stage. In the majority, the published accounts that exist are clinicians writing up series of single case studies (Harvey, 1994; Denman, 1995; Treasure & Ward, 1997) alongside the findings of a couple of small RCTs looking at the value of CAT in treating anorexia nervosa (Treasure, Todd, Brolly et al.,1995; Dare, Eisler, Russell, Treasure, & Dodge, 2001).
This limited evidence base is reflected in the current NICE Guidelines for the treatment of people with eating disorders (2004), which make reference to the potential value in using CAT in treating anorexia nervosa but does not include CAT in its recommendation for the treatment of bulimia nervosa or ‘eating disorders not otherwise specified’ (EDNOS). Tanner and Carolan’s (2009) audit of 100 patients treated with CAT however highlight the potential for CAT to be used across a range of patients with eating disorder presentations. Their findings demonstrated significant improvement in symptoms in both patients with anorexia and bulimia at the end of therapy.
The NICE Guidelines (2004) recommend that any psychological therapy offered should be focused upon the eating difficulties. Treasure & Ward (1997) highlight how CAT can maintain this focus by ensuring that target problems include issues such as low weight and dietary restriction, but also allows for a focus on other issues that may be maintaining the eating disorder. For example, in bulimia, a pattern of “striving and following the rules” resulting in “unmet needs and a sense of deprivation” can trigger an episode of “rebellion quickly followed by guilt and self-criticism”. Such a procedural pattern can be useful in thinking through the factors that maintain a binge-purge cycle and that may also be impacting upon other aspects of the individual’s life and relationships.
Some particular areas, which I believe CAT is well equipped to address are the interpersonal (Schmidt, Tiller, Blanchard, Andrews, & Treasure, 1997) and emotional difficulties (Troop, Schmidt, & Treasure, 1995) commonly reported by clients with eating difficulties. A number of studies have reported a higher incidence of personality disorders (61%), including borderline personality disorder (25%) with clients with bulimia (Schmidt & Telch, 1990; van Hanswijck de Jonge, van Furth, Lacey & Waller, 2003). The NICE guidelines acknowledge that clients with such presentations are less likely to respond to a standard programme of CBT / IPT treatment and recommend that treatment should therefore be adapted to the problems presented. CAT, as a relational therapy, is therefore a strong contender in such cases. In particular, I find the SDR can be very useful in helping clients to understand and recognise both impulsive behaviours and the dissociated states that may be associated with them. In my experience, clients presenting with such difficulties benefit from a longer 24 session CAT as would be recommended for clients with borderline personality disorder (Ryle, Leighton, & Pollock, 1997). A good account of the rationale and method of using CAT to work with clients who have such difficulties is in Ryle et al’s (1997) text on using CAT with borderline personality disorder.
The NICE Guidelines also recommend that outpatient psychological treatment for anorexia nervosa should normally be of at least six months duration. A review of using CAT to treat eating disorders (Tanner & Connan, 2003) makes reference to the comparative brevity of CAT as a potential disadvantage in this regard, but also highlights how the time-limited nature of the approach can be useful in ensuring that endings are well managed as they are focused upon from the start; an aspect of particular importance when separation and dependency issues are apparent. In my own practice, I have moved towards offering low weight clients with anorexia nervosa a 24 session CAT followed by monthly reviews for three months and then further review three months later. This then provides clients with a package of support, which spans over approximately 12 months.
For bulimia nervosa, the NICE Guidelines recommend a course of 16-20 CBT sessions over four to five months. Whilst for IPT, they recommend that similar outcomes will require intervention over a period of 12 months. These recommendations may just reflect differences between the two approaches, but as they were compiled from various sources of evidence, they may also reflect some variation between the clinical populations that were offered the respective treatments. In terms of offering CAT to clients with bulimia, I tend to offer a 16 session CAT to the majority of clients presenting with a first episode and find this to be sufficient. However, for more complex cases with co-morbid difficulties a 24 session CAT is often more appropriate.
Reflections on Practice
Common reciprocal roles and procedural sequences
Some of the characteristics well associated with clients who have eating disorders in the literature (e.g. perfectionism, low self-esteem, placation, limited sense of autonomy, impulsivity) can be usefully mapped onto recognised reciprocal roles and procedural patterns. I will describe my own experience of using CAT with patients with these RRPs and compare it with some of my clinical experience of this group of patients using CBT.
Perfectionism & Low self-esteem
Perfectionism is a personality trait that has long been considered a risk factor for eating pathology (see Wonderlich, 2002; Shafran, Cooper & Fairburn, 2002). It promotes the relentless pursuit of the ‘thin ideal’ in anorexia nervosa and Fairburn (1997) suggests that perfectionism is a maintenance factor for bulimic pathology as it encourages the practice of rigid dieting that is thought to underlie the binge-purge cycle. It is recognised that perfectionist patterns may also relate to other aspects of the life of people with eating disorders such as their performance at work or sport, alongside attempts to control their eating, shape and weight.
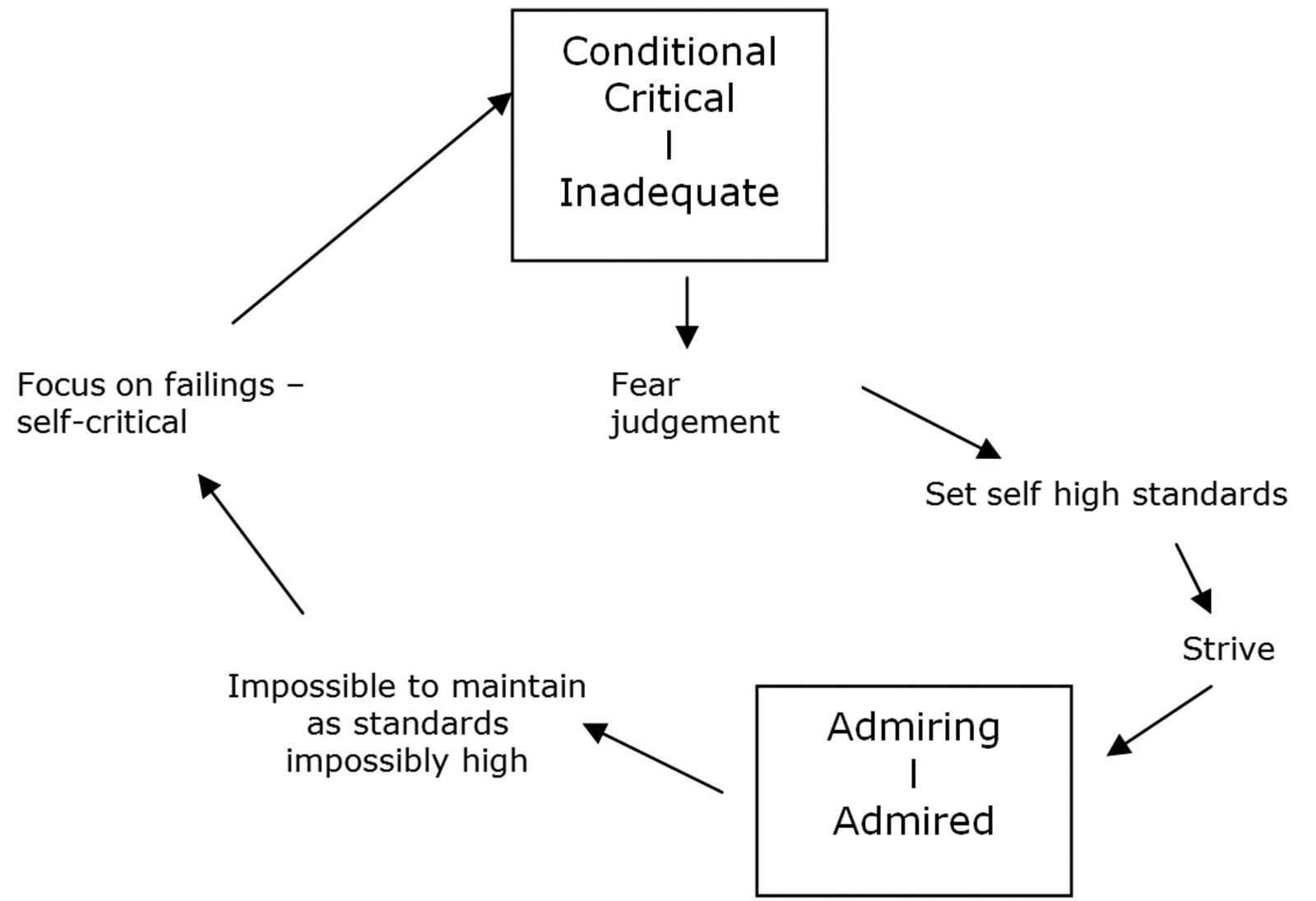
As a procedural pattern, perfectionism often seems to relate to a reciprocal role of conditional / critical care and a fear of being judged inadequate. The striving response reflected in a perfectionist pattern however embodies this reciprocation, as high standards are set and the individual is orientated towards noticing perceived failings as opposed to achievements. This in turn drives the cycle, as detailed in the following diagram.
Whereas in CAT this is formulated as a procedural pattern, in a CBT formulation a similar cycle is often mapped out in a series of thoughts, feelings and behaviours stemming from a set of core beliefs and assumptions. Certainly, this was a pattern that I felt familiar with prior to using CAT to inform my work. Using a CBT model however, I was often prone to focusing in too great a detail on specific sets of assumptions and beliefs, lessening the opportunity to step back and observe the pattern from a more reflective position.
CAT has provided me with tools to encourage this process of reflection with my clients. Mapping out an SDR with a client can help them see how the high standards that they set for themselves are maintaining this cycle – and the pattern can be described in a sufficiently broad way so as to encompass enactments of similar RRPs beyond the disordered eating.
One of the clear advantages of the CAT model is the flexibility of the SDR in illustrating how an enactment may take place within the therapy. In particular, I have noticed how much more able I am as a therapist to reflect on how I may be being drawn into a client’s procedural pattern when working using a CAT model.
The special admiring-admired state is one which therapists working with this client group can easily be drawn into. In the past, I have noticed a strong draw to ‘rescue’ clients and be the one to offer the understanding that they frequently report lacking in their other relationships. However as the previous diagram highlights, this special admired place can be a fragile one, and as a consequence, therapists may be drawn into colluding with clients for fear of losing this position. This can result in difficulties such as the therapist endorsing unrealistic goals that the client may have in terms of ideal weight / shape as opposed to challenging these through helping the client to identify them as impossible to achieve.
I believe that the fragility of the special admired place is also a key factor in understanding how individuals can shift from applying this procedural pattern in various other aspects of their lives to increasingly becoming preoccupied with their weight, shape and eating. In my work, clients will often describe how their eating disorder initially provided them with a sense of mastery and control, whereas striving within other areas of their lives was often complicated by factors beyond their control. They are therefore drawn to the apparent simplicity of weight loss through restriction or purging. Again this is an illusion both because of the impossible standards they try to reach but also because the body’s physiological response to malnutrition increasingly threatens this position.
In my clinical work, I find there is a role for psycho-education in relation to this: Although clients often have a vast knowledge of the calorific contents of foods they rarely understand the impact that inadequate or infrequent eating has both upon their metabolic rate and their cognitive and emotional wellbeing (in terms of increased preoccupation with food, social withdrawal, increased anxiety and reduced mood). Understandably these physiological responses often drive the eating disorder cycle further as they represent a threat to both the striving eating disordered pattern but also to other arenas in which the procedural pattern may have been taking place. This is often a factor in the increasingly harsh ‘eating rules’ individuals develop in an attempt to regain a sense of control and mastery.
One aspect of working with people with eating difficulties that is a common arena for such enactments is the process of monitoring weight. This is particularly an issue for clients with anorexia nervosa, where NICE guidance clearly states that the delivery of psychological interventions should be accompanied by regular monitoring of a patient’s physical state including weight and specific indicators of increased physical risk. However I think regular weight monitoring can be a useful feature of working with clients with a range of eating difficulties as I believe it is unreasonable to expect someone to make changes to their eating patterns (e.g. having regular meals as a way of reducing the physiological urges to binge eat) without them having the feedback loop to address the fears they hold about how this change may affect their weight.
Since using CAT formulations in my work, I have found that it is easier to explicitly address the potential for clients to have mixed feelings in relation to this trap. Using the SDR, clients have been able to describe two conflicting loops: – one of fearing judgement for weight gain from their internal ‘anorexic’ voice and the other fearing judgement from therapists or family for ‘not making progress in recovery’. This has helped me reflect on previous cases where there was a sense of appeasement in the way clients described feeling distressed and surprised at any weight loss, despite a fear of weight gain being an acknowledged part of their eating disorder.
Such placation can make it difficult for therapists to accurately judge where clients are in terms of their readiness to change. For example, clients will sometimes express concern over their low weight in order to comply with the perceived expectations of the therapist, which can draw therapists into assuming that weight gain is a shared goal. Such a pattern may increase the likelihood of therapists finding it hard to remain neutral in their response to weight change, especially when working with very underweight clients. This can then make it difficult for clients to share their true feelings about these matters. Obviously, these patterns can be present regardless of the therapeutic approach of the clinician. However I have found that the CAT model particularly helpful in enabling explicit discussion of what may be happening in these instances.
Placation and a limited sense of control
As I have previously described, a patterns of placation, ‘trying to please’ or ‘avoid hurting others’, can be closely related to the perfectionist ‘striving’ pattern. One consequence of these patterns can be a reduced sense of autonomy, which the individual tries to compensate for by seeking a sense of control through their relationship with food.
A further aspect, which can drive this pattern is the response of others to the client’s eating disorder. The sense of control that the client may try to gain through disordered eating often leads to increased anxiety in others close to them. This may, in part, be an attempt to elicit care if the client has previously experienced a lack of care. However, the concerned response of others can also often be experienced in a negative way. Often clients will describe feeling that all their friends / family seem concerned about is whether they have eaten, not actually how they are. Obviously this pattern can frequently emerge in therapy, especially when a client’s eating disorder is presenting a considerable risk to their health: for example, a process of meal planning in a therapy session can result in the therapist taking on an anxious directive voice akin to that of a parent at home.
Some of these patterns have been drawn out in the following diagram:
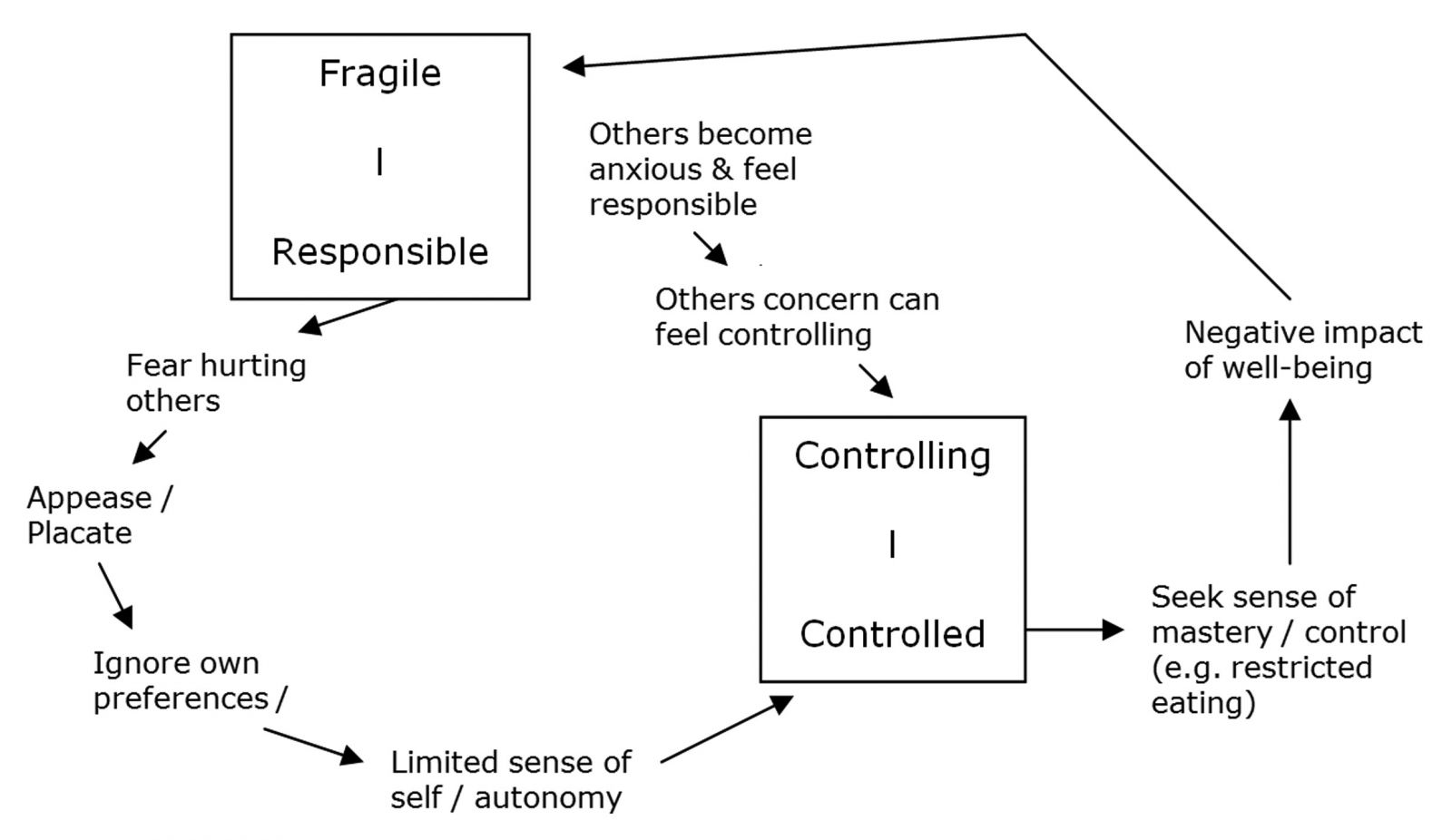
As the diagram highlights, the response of others to eating disordered behaviour can often feed into a procedural pattern, which further reduces a client’s sense of autonomy. This may lead to an increased need to seek autonomy via their eating disorder, or may also develop into an alternative pattern of rebellion with ‘If I must not, I will’ responses. Such patterns can also be useful in understanding the bingeing behaviour associated with purging anorexia and bulimia nervosa.
It is important for clinicians to be aware of the potential for these patterns within the therapy, particularly as they may feel a sense of responsibility for their client especially if their health is fragile. Certain aspects of therapeutic work can also act as ‘enactment magnets’. An example is the use of food monitoring sheets in which clients record what they have eaten and the context of eating (where, when, how they were feeling, what thoughts they were having). These are central to the CBT approach to managing eating disorders, and research does indicate a significant relationship between regular monitoring and positive outcome in terms of regulating meal patterns (Fairburn, 1995). Monitoring has clear benefits in terms of helping therapist and client to reflect on eating patterns and to identify particular food rules the client may be adhering to and the stress factors that trigger periods of restriction or binge eating. As clients are encouraged to complete their monitoring throughout the day as opposed to retrospectively at the end of the day, it can be a useful tool in helping a client develop an ‘observing eye’ and reflect on what is happening from a more distanced perspective. Following reformulation and the development of an SDR, I often encourage clients to use these same sheets to track TPPs.
The monitoring process can be quite a magnet for enactments involving versions of either critical-criticised or controlling-controlled reciprocal roles. Left unaddressed, these potentially can become destructive and undermine the therapeutic alliance. Where relevant, having these made explicit on the SDR and working collaboratively with a client to help identify when related patterns are being enacted is highly valuable. I have found that the very act of this process can be a helpful way of, at least temporarily, ‘stepping out’ of the enactment.
The relationship between eating behaviours and difficult feelings
The relationship between emotion and eating difficulties is well recognised and a component of a variety of interventions. Formulating the interaction between eating difficulties and difficult feelings is an important part of any therapeutic work. Much of my clinical work, when using a CBT approach, was focused on using monitoring sheets to help identify the contexts which acted as triggers for episodes of food restriction or binges / purges. One challenge to this work was where clients presented with a very limited capacity for self-refection and were often left struggling to identify what they were feeling. Often in these cases, food restriction or more commonly binge and purge episodes were used in combination with other self harming behaviours such as cutting, alcohol or substance misuse and served a functional role of numbing feelings often to the point of dissociation.
Conclusion
I feel that CAT has a considerable amount to offer clinicians working with clients presenting with eating difficulties. In particular, I feel that the model is well equipped to formulate and work on issues integral to the eating disorder alongside broader interpersonal difficulties. As I have reflected on earlier, TPPs such as ‘people pleasing’ can often be used to both map out a client’s behavioural response to their critical anorexic thoughts alongside their interactions with others (including yourself as their therapist).
CAT therefore provides clinicians with tools that can help address some of the enactments, which are inevitably going to take place within the therapeutic relationship. Within the day service component of the eating disorder service I work in, we have found it useful to have a CAT formulation developed for each of the day service attendees. Alongside informing clients’ care plans, this has proven to be a highly valuable framework in helping the team reflect on the different interactions clients have with the various members of staff and helped manage the potential for splitting within the team.
CAT as a model also has the flexibility to be used alongside techniques from other approaches, such as CBT based monitoring, that I have previously found useful. Once again, I find the usefulness of these techniques is enhanced by having a formulation that allows for discussion and reflection on any enactments that may take place during their use.
Dr Amy Wicksteed, Chartered Clinical Psychologist, CAT Practitioner
I am currently work as a Clinical Psychologist for Sheffield Eating Disorders Service. I have been using CAT within my work for the past 10 years, and qualified as a CAT Practitioner in 2007.
Correspondence: Sheffield Eating Disorders Service, St Georges Community Health Centre, Sheffield, S3 7ND. Email: Amy.Wicksteed@SHSC.nhs.uk
References
Dare, C., Eisler, I., Russell, G., Treasure, J., & Dodge, L. (2001). Psychological therapies for adults with anorexia nervosa: randomised controlled trial of out-patient treatments. British Journal of Psychiatry, 178, 216-221.
Denman, F. (1995). Treating eating disorders using CAT: two case examples. In A.Ryle (Ed), Cognitive Analytical Therapy: Developments in Theory and Practice. Chichester: Wiley.
Harvey, L. (1994)… CAT and Eating Disorders. ACAT News, 31st March 1994.
Fairburn, C. G. (1997) Interpersonal psychotherapy for bulimia nervosa. In Handbook of Treatment for Eating Disorders (2nd edn) (eds D. M. Garner & P. E. Garfinkel), pp. 278-294. New York: Guilford.
Fairburn, C.G. (1995) Overcoming Binge Eating. Guilford Press. London.
National Collaborating Centre for Mental Health. (2004). Eating Disorders: Core interventions in the treatment and management of anorexia nervosa, bulimia nervosa and related eating disorders. Clinical Guideline 9. London, UK. National Institute for Clinical Excellence.
Ryle, A., Leighton, T., & Pollock, P. (1997). Cognitive Analytic Therapy and Borderline Personality Disorder: The Model and the Method. Wiley, London.
Schmidt, N.B., & Telch, M.J. (1990). Prevalence of personality disorders among bulimics, non-bulimic binge-eaters, and normal controls. Journal of Psychopathology and Behavioral Assessment, 12, 169-185.
Schmidt, U., Tiller, J., Blanchard, M., Andrews, B., & Treasure, J. (1997). Is there a specific trauma precipitating anorexia nervosa? Psychological Medicine, 27 (3), 523-530.
Shafran, R., Cooper, Z., & Fairburn, C. G. (2002). Clinical perfectionism: a cognitive-behavioural analysis. BehaviourResearch and Therapy, 40, 773–791.
Tanner, C. & Connan, F. (2003). Cognitive Analytic Therapy. In Handbook of Eating Disorders. Edited by J. treasure, U Schmidt., & E. van Furth. John Wiley & Sons Ltd. London.
Tanner, C. & Carolan. A. (2009). Audit of Cognitive Analytic Therapy Cases in Eating Disorders. Presented at the 2009 International ACAT conference.
Troop, N.A. Schmidt, U.H. & Treasure, J. (1995). Feelings and fantasy in eating disorders: a factor analysis of the Troop Alexithymia Scale. International Journal of Eating Disorders, 18 (2), 151-157.
Treasure., J. Todd, G. Brolly, M. Tiller, J. Nehmed, A., & Denman, F. (1995). A pilot study of a randomised trial of cognitive analytical therapy vs educational behavioural therapy for adults with anorexia nervosa. Behaviour Research and Therapy, 33 (4), 363-367.
Treasure, J. & Ward, A. (1997). Practitioner Report: Cognitive Analytical Therapy in the Treatment of Anorexia nervosa. Clinical Psychology and Psychotherapy, Vol. 4 (1), 62-71.
van Hanswijck de Jonge, P. van Furth, E.F. Lacey, H.J. & Waller, G. (2003). The prevalence of DSM-IV personality pathology among individuals with bulimia nervosa, binge eating disorder and obesity Psychological Medicine, 33: 1311-1317, Cambridge University Press
Wonderlich, S. A. (2002). Personality and eating disorders. In C. G. Fairburn, & K. D. Brownell (Eds.), Eating disorders and obesity: a comprehensive handbook (2nd ed.) (pp. 204–209). New York: Guilford Press.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Wicksteed, Dr. A., 2012. Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice. Reformulation, Summer, pp.26-31.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
CAT and Eating Disorders
Harvey, L., 1994. CAT and Eating Disorders. Reformulation, ACAT News Spring, p.x.
Perfectly Imperfect: Reflections of a Newly Qualified Clinical Psychologist in using CAT to Explore the Relational Contribution to Binge Eating
Dr Lyndsey Holt, 2017. Perfectly Imperfect: Reflections of a Newly Qualified Clinical Psychologist in using CAT to Explore the Relational Contribution to Binge Eating. Reformulation, Winter, pp.28-32.
CAT and Obesity: My Reflections
Hill, L., 2015. CAT and Obesity: My Reflections. Reformulation, Winter, pp.8-9.
CAT Effectiveness: A Summary
Quraishi, M., 2009. CAT Effectiveness: A Summary. Reformulation, Summer, pp.36-38.
A Little Italian Story – Service Development
Fiorani, C., Poggioli, M., 2009. A Little Italian Story – Service Development. Reformulation, Summer, pp.13-14.
Other Articles in the Same Issue
A Hopeful Sequential Diagrammatic Reformulation
Bradley, J., 2012. A Hopeful Sequential Diagrammatic Reformulation. Reformulation, Summer, pp.13-15.
Aims and Scope of Reformulation
Lloyd, J. and Pollard, R., 2012. Aims and Scope of Reformulation. Reformulation, Summer, pp.3-4.
CAT with People who Hear Distressing Voices
Perry, A., 2012. CAT with People who Hear Distressing Voices. Reformulation, Summer, pp.16-22.
Great Time: From Blade Runner to Bakhtin
Pollard, R., 2012. Great Time: From Blade Runner to Bakhtin. Reformulation, Summer, pp.32-34.
Letter from the Chair of ACAT
Hepple, J., 2012. Letter from the Chair of ACAT. Reformulation, Summer, p.6.
Letter from the Editors
Lloyd, J. and Pollard, R., 2012. Letter from the Editors. Reformulation, Summer, p.5.
Reflections on a Dilemma in a Supervision group: Caught between a Rock and a Hard Place
Gil-Rios, Dr. C., M., and Blunden, Dr. J., 2012. Reflections on a Dilemma in a Supervision group: Caught between a Rock and a Hard Place. Reformulation, Summer, pp.23-25.
Sleep Tight: Working Creatively with Dreams in CAT
Coulter, N. and Rushbrook, Dr S., 2012. Sleep Tight: Working Creatively with Dreams in CAT. Reformulation, Summer, pp.7-12.
The 16 + 1 interview
Petratou, V., 2012. The 16 + 1 interview. Reformulation, Summer, p.43.
Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice
Wicksteed, Dr. A., 2012. Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice. Reformulation, Summer, pp.26-31.
What is the 2005 Mental Capacity Act and how can CAT help us to make sense of the decision making process at its heart?
Brown, H. and Lloyd, L., 2012. What is the 2005 Mental Capacity Act and how can CAT help us to make sense of the decision making process at its heart?. Reformulation, Summer, pp.35-42.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.