Reciprocal roles within the NHS
Welch, L., 2012. Reciprocal roles within the NHS. Reformulation, Winter, pp.14-18.
Introduction
The commercialisation and privatisation of the National Health Service at the global, political level or in local workplace settings triggers feelings of despair and hopelessness, undermining the vital task of building ways of defending a hugely important service. Whilst a political-economic explanation of the changes is essential to grasp both the profit motivated drivers behind the changes and the social values underpinning opposition, the concept of reciprocal roles offers a valuable additional component for understanding how authoritarian directives lead to a largely compliant response. The difficulty with exploring reciprocal roles in the NHS is that it means connecting the diverse ‘domains’ which are fundamental to an integrated understanding; namely, at the macro level, the Political-Economic and at the micro level, the Social-Psychological. Each domain, on its own, provides only a partial understanding; awareness of the interconnections is vital in considering what actions may be effective in opposing the undemocratic dismantling of the NHS. One of the problems is that each domain draws on a vast range of complex knowledge and it is very easy to interpret another domain within the language of the one we are more familiar with. From a political perspective, individuals can be portrayed as carriers of social structures and a psychological position can be dismissed as self indulgent, a diversion from the real issues, while, from a psychological perspective, the social is often seen as the individual writ large and political issues are considered an evasion of real emotional issues. It is vital to recognise the interrelationship as well as distinctions between the different domains: the concept of reciprocal roles is highly valuable in the Social-Psychological domain and may well provide a fruitful tool in the Political-Economic but it cannot replace for example, the vital statistical information that is so necessary to grasping how money is exchanged in the financial arena. Lucien Sève expresses the connectedness between the domains: “many political problems consist at least in part of a psychological problem which arises for millions” (Sève, 1978, p13). In this short article I start with a very brief account of the role of the economic in shaping the political decisions in relation to the NHS. I then give an overview of reciprocal roles and how an exploration of this area opens an arena neglected by the political domain that is crucial in building a sense of solidarity and connectedness amongst those who oppose the privatisation of the NHS.
Politics and Economics
The 2012 Health and Social Care Act opened the floodgates for the whole scale privatisation of the NHS, a process started by the creation of the internal market by Thatcher in 1989 and built on by the start of Foundation Trusts by Blair in 2004 (the impact of the Foundation Trusts in mental health services is described well by Jones & Child (2007)). The Secretary of State no longer has a duty to provide a national health service, undermining a principle fundamental to the birth of the NHS in 1948. Neither the Tories nor the Lib-Dems argued for these changes in their 2010 general election campaigns and their initial coalition agreement made no mention of it. Such a huge change without a public mandate, undermines the notion of democracy in the United Kingdom, and makes explicit the dominance of the values of those who own and control wealth in society, above those of the mass of the voting population.
The scale of change can easily be experienced as overwhelming, eliciting reciprocal role responses of impotent fury (it’s outrageous) followed by despair (there is nothing I can do about it) or indifference (we just have to get on with it). Building effective opposition is not an easy process but I believe it can be strengthened and enhanced if we can deepen our understanding of how it has come about.
There are of course many entries into the political-economic domain. A recent study by Coghlan & MacKenzie (2011) gives an interesting snapshot into the hidden dimension of the economic domain. Their study of a database of 37 million companies and investors worldwide, identified 43,060 Transnational Companies (TNCs) and the share ownerships linking them. They found a core of 1318 companies with interlocking ownerships connecting them to, on average, 20 other companies. They describe 147 of these companies, less than one percent of the total, as a “super-entity” controlling 40 percent of the entire network. The top 20 of the 147 superconnected companies include Barclays plc, Capital Group Companies Inc, AXA, Legal & General Group plc, Merrill Lynch & Co Inc, Credit Suisse Group, Goldman Sachs Group Inc.
The impact of large companies on the NHS has been illustrated by the website, www.powerbase, which shows links between different companies and the top echelons of government: Cameron, Lansley and before them, Blair. These companies include Capita, Care UK, Circle, Kaiser Permanente, KPMG, Lilly, Pfizer, Roche, and United Health. The Daily Mail (Rose, D (12 Feb 2012)) (not a paper I normally read!) gave a powerful description of the influence of one of these companies, McKinsey, in shaping the Health and Social Care Act. McKinsey is worth more than £4 billion and its clients include 15 of the world’s 22 largest healthcare and drugs firms. Many of the Health & Social Care Act proposals, which open up most of the current £106 billion NHS budget to the private sector, were drawn up by McKinsey and included in the legislation wholesale. McKinsey worked closely with the last Labour Government on health, and produced a 2009 report recommending the NHS cut ten per cent of its staff. Since the Coalition took office, the company earned at least £13.8million in forming Government health policy. McKinsey used its privileged access to ‘share information’ with its corporate clients who are now set to bid for health service work. The intricate interconnections between so-called ‘public’ bodies and private companies is illustrated graphically in a micro example by David Bennett, the head of the NHS regulator, Monitor, who 8 years ago was an employee of McKinsey and in June 2011 he spent a business weekend in New York at the cost of £6,200 courtesy of McKinsey. The intimate links between individual representatives of powerful companies and the political establishment has been central to weaving the web of commercial interests into the public sector in a language whose surface is littered with phrases seen to be in the interests of building a better service, such as modernising, improving and patients’ choice.
The rhetoric of the necessity for the £80 billion of cuts in the public sector needs to be placed in the context of the £120 billion lost each year in tax avoidance and non collection of tax. In 1948, when the NHS was created, the national debt was £240 billion; now it is £50 billion.
Social and Psychological
The macro level of the political and economic is built on dominance at the micro level of relationships amongst the population at large and, in this topic, amongst NHS staff. It is perhaps useful first to give a brief account of how a ‘cellular’ level of relationships operate in a highly simplified form which can then be connected to the Political-Economic domains. We have immediate ‘fast brain’ quick reactions and thoughtful, slow brain responses to each other and to objects in the world (Kahnemann 2012). These lead to actions, as a result of which give us the possibility of reflecting and learning. The strength of the psychotherapeutic understanding of reciprocal roles lies in focussing especially on their development within early and childhood relationships. What is absent from the psychotherapeutic analysis is the creation and exchange of products: human labour is central to understanding the development of humans. Our wage in exchange for our work is vital in enabling us to sustain our lives and anxieties about its loss can powerfully shape our responses to changes in the workplace. The ownership and control of the objects humans produce or the services delivered, however, lies in the hands of the rich and powerful whose financial judgements about how to increase their wealth makes them deaf to the needs of the workforce and to the population at large. It usually takes acute crises for the working population to begin to assert their own needs independently from those above them who direct their activities.
The ‘cellular’ level of relationships operate primarily at the level of personal, family relationships, friendships, local community and colleagues at work where our actions and responses usually effect one other person, or a small group. We experience political reciprocal roles at a deep unconscious level, unaware of the power of the super-rich. A very narrow view of the world is presented to us by those in positions of authority over us or through the media, subtly shaping the language we use and our concepts and knowledge of the world. This ‘primes’ (Kahnemann 2012) us to think using our fast brain responses rather than encouraging us to think slowly and see how power relationships play a fundamental role in the workplace. In a series of interviews, Board & Fritzon (2005) examined the mental health in high level executives compared with patients in Broadmoor, finding a greater prevalence of histrionic, narcissistic and obsessive compulsive personality disorders, leading them to describe the executives as “successful” psychopaths compared with the “unsuccessful” ones in prison.
This highly intricate web of relationships is shaped by those in positions of power in the NHS who cascade downwards the directives they receive from those above, demanding acceptance of edicts by those in the lower echelons. The fast brain reciprocal role responses all too often trigger an unthinking compliance, a sense that this is the world we have to accept.
Two meanings come together in one phrase: “we’re in this together” gives an appearance of connectedness, equality; the feeling that differences between us are insignificant when faced with difficulties of the economy. The complete emptiness of the phrase is demonstrated by pivotal differences in wealth where the rich and super-rich are only too happy to avoid paying tax while demonising those on benefits. “Patients’ choice” is something we would all support on the surface but the real meaning for those in power is about creating competition amongst hospitals, not providing open accessible care to all. The hollowness of the rhetoric of putting GPs and frontline staff in charge of commissioning is quickly revealed when private companies are brought in to administer the complex, expensive bureaucracy required by this new system. The dual meanings are powerfully demonstrated by Circle’s ex-banker boss, Ali Parsa, who says “we believe our partners – the doctors, nurses and healthcare professionals – should run their own hospitals” (Hamer, 2012). After Circle took over the Hinchingbrooke Healthcare Trust in February, they went on to make cuts in nursing posts and the cleaning budget. Can it really be believed that the staff would agree with this?
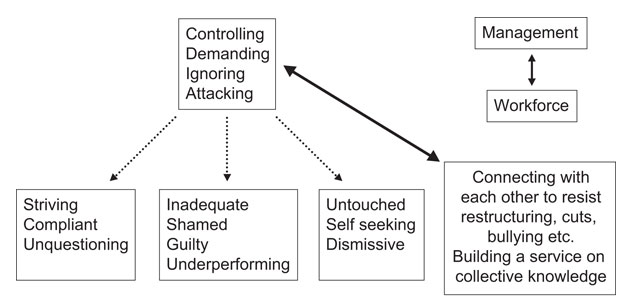
Increasingly the deeply human service provided in health care is reduced to the language of numbers as the addiction to performance indicators becomes the central driver for judging the services delivered; a key factor in these numbers is the language of finance and money. The imperative for managers in the NHS is to drive, control and criticise the workforce to work more ‘productively’ for less pay. Their focus is on numbers: finance, statistics and targets directing their immediate, non-thinking responses to those below them. Private independent consultants are brought in to reconfigure services largely ignoring the intimate knowledge the workforce has of how the service operates in practice.
All too often the reactions to commands from above range from conscious agreement to unthinking compliance (“this is how the world is, get on with it”). This merges into resigned acceptance or silent protest of something experienced as disturbing. It is very easy to experience the instructions as just that and to feel impotent. NHS management increasingly promotes a sense that dialogue and discussion present unnecessary delays; managers become focused on ensuring that the directives they are carrying out are complied with by those beneath them. Genuine discussion amongst adults about complex issues is dismissed as time wasting. Generally the views of the workforce are seen as irrelevant; although at times changes are given the gloss of ‘consultations’ (see also Jones & Childs (2007)), the majority of these are meaningless exercises though at least they can slow the process down. Becoming assertive in the face of this is not an easy process for the workforce and probably more so for those who work psychotherapeutically as the nature of the work requires listening to the views of others and responding sensitively in a way that aims to help the patient to think about themselves. In contrast, responding to managers requires a very different mental state of assertion not accommodation, expressing an independent viewpoint rather than seeking to reach a shared conclusion as there is a fundamental divide between the participants in this debate. At a minimum, for those working psychotherapeutically to help patients make fundamental changes in their lives, discovering how our own micro level reciprocal roles interfere with our capacity to speak as adults to those in authority over us can at least build our understanding of why it can be so difficult for patients to make real shifts.
What can be done?
The most basic ‘change’ is at the micro level of recognition that what is being done to the NHS has no democratic mandate. It is also about being alert to the superficiality and double meanings espoused in many NHS policies which on the surface promote values that we are all committed to but in practice are used to speak the wishes of management, not the workforce. Any change starts with forming a new awareness of reality as it presents itself to us. This requires fostering a sense that the views held at the workforce level have legitimacy and that the deep unconscious parent-child or teacher-pupil reciprocal roles which can so easily be triggered by the latest management directive need to be brought into conscious awareness in order to make possible a sense that the most effective service will be the product of adult-adult dialogue.
Awareness alone is of course insufficient to bring about change though it is the essential beginning. Discussion with family, friends and colleagues is vital to deepening the awareness that the ‘modernization’ of the NHS must be opposed. Fortunately as the ‘modernisations’ dig more deeply into the NHS, we are beginning to get expressions of disagreement and dialogue with colleagues. Occasionally there is even a refusal to comply in solidarity with others. An increasing number of websites have set up petitions helping to give collection expression to this opposition. Trade unions and political groups like ‘Keep Our NHS Public’ are vital in organizing opposition.
In the further future it is also of great importance that we find ways of articulating alternatives to how the NHS is currently run by financial targets set by those at a great distance from the workplace. This requires that we deepen our psychotherapeutic knowledge of collaboration in order to construct democracy in the workplace. Democracy has to be asserted and regained in the political domain but we also need to think about how it can be a powerful tool in the workplace, engaging those who do the work in the task of developing and improving the services we offer. Chief executives should be elected, not appointed by representatives of those above them; salary scales should be proportional so that the highest paid have limits placed on what they earn, determined by the wage received by the lowest paid. This could be, say, 10 times or, at the most, 20 times the lowest paid worker. The ‘reward’ of hard work should surely be the satisfaction that it is successfully helping patients, not the number of zeros achieved in a pay package.
For democracy in the workplace to be successful, many tools would be needed. The problems can be seen particularly in the way the political Left is organized, where differences between individuals often become large barriers in building up effective links between different political groupings. While there is probably general agreement among the Left that the wealth divide (e.g. 1210 global billionaires owning $4.5 trillion of wealth compared with $8.5 trillion owned by the 3.01 billion adults with net worth less than $10,000) has to be broken for serious social change to take place, there are inevitably many different viewpoints on how this should be challenged and what the world might look like in the future. These divisions are hardly surprising given the complexity of the problem and the unknown nature of the future but those on the Left need to be able to discover ways of hearing each other’s viewpoint rather than losing sight of commonalities and focusing solely on the differences. This is not an easy process as can be illustrated by a strike in a workplace. The risks taken by the strikers and their loss of pay can make it very difficult to maintain relationships with those who choose not to strike. We also need to recognize that there will be some who support the commercialization of the NHS who will be impervious to our viewpoint; we have to ensure that our arguments are solidly grounded in order to minimize the chances of others being won over to the other side.
The concept of reciprocal roles could form a strong basis for the development of democracy through awareness that our fast emotional reactions to others can easily over-ride our capacity to hear clearly what the other is saying. Our assumed knowledge of an area can make us super confident so that we quickly dismiss another’s differing viewpoint. Developing observing selves could open up space for dialogue between those who are working at a broadly equal level. While it is possible for those in authority to hear the views of those beneath them, the likelihood of this will be much less, particularly at middle management level which is subject to powerful commands from above.
Conclusion
A short article inevitably summarizes too briefly the highly complex interaction between the micro social-psychological domain and that of the political-economic, but I hope it provides a space to consider one of the many ways in which effective opposition to anti-democratic replacement of the NHS by one modeled on the US can be built. I would be interested in any comments that readers might have to the article: c.lawrencewelch@gmail.com
Biography
Dr Lawrence Welch is a founder member of ACAT, a trainer and supervisor in ACAT North and a Consultant Psychotherapist working in the NHS psychological therapies service in North Tyneside.
References
Board, Belinda Jane & Fritzon, Katarina 2005, ‘Disordered personalities at work‘ by, published in Psychology, Crime & Law, Volume 11, Issue 1 March, pp 17 – 32.
Coghlan, A. & MacKenzie, D. 2011, Revealed – the capitalist network that runs the world. New Scientist 2835
Hamer, T. 2012, Stop these parasites! Solidarity & Workers Liberty, 22 August, no 254
Jones, A. & Childs, D. 2007, Reformulating the NHS reforms.Reformulation, Summer pp 7-10
Kahneman, D. 2012, Thinking Fast and Slow, Penguin
Rose, D. 2012, NHS health reforms: Extent of McKinsey & Company's role in Andrew Lansley's proposals. 12 Feb, Mail Online.mht
Sève, L. 1978, Man in Marxist Theory and the Psychology of Personality, Harvester Press
Websites
Keep our NHS Public www.Keepournhspublic.com
HealthAlarm www.healthalarm1159.wordpress.com
www.Nhsunity.com
http://www.powerbase.info/index.php/Health_Portal
www.38degrees.org.uk
www.Axetheact.org
www.Avaaz.org
www.Falseeconomy.org.uk
www.inequality.org
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Welch, L., 2012. Reciprocal roles within the NHS. Reformulation, Winter, pp.14-18.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Politics, Reciprocal Roles and Dialogue
Welch, L., 2014. Politics, Reciprocal Roles and Dialogue. Reformulation, Winter, pp.6-8.
Psycho-Social Checklist
-, 2004. Psycho-Social Checklist. Reformulation, Autumn, p.28.
Private Misery, Public Rage and Poor Soundproofing - Seeking Happiness in the NHS
Welch, L., 2000. Private Misery, Public Rage and Poor Soundproofing - Seeking Happiness in the NHS. Reformulation, ACAT News Summer, p.x.
Letters to the Editors: New, Modern, Dependable?!
Welch, L., 2003. Letters to the Editors: New, Modern, Dependable?!. Reformulation, Summer, pp.9-10.
CAT in the NHS: Changes as a result of the Health and Social Care Act 2012 and the future of CAT
Vesey, R., 2012. CAT in the NHS: Changes as a result of the Health and Social Care Act 2012 and the future of CAT. Reformulation, Winter, pp.6-9.
Other Articles in the Same Issue
A letter to the NHS...
Anonymous, 2012. A letter to the NHS.... Reformulation, Winter, pp.20-21.
Aims and Scope of Reformulation
Lloyd, J. and Pollard, R., 2012. Aims and Scope of Reformulation. Reformulation, Winter, p.45.
Anonymous Letters
Anonymous, 2012. Anonymous Letters. Reformulation, Winter, pp.22-23.
Book Review: Post Existentialism and the Psychological Therapies: Towards a therapy without foundations
Pollard, R., 2012. Book Review: Post Existentialism and the Psychological Therapies: Towards a therapy without foundations. Reformulation, Winter, p.43.
CAT in the NHS: Changes as a result of the Health and Social Care Act 2012 and the future of CAT
Vesey, R., 2012. CAT in the NHS: Changes as a result of the Health and Social Care Act 2012 and the future of CAT. Reformulation, Winter, pp.6-9.
Cognitive Analytic Therapy & Dysphagia: using CAT relational mapping when teams can’t swallow our recommendations
Colomb, E. and Lloyd, J., 2012. Cognitive Analytic Therapy & Dysphagia: using CAT relational mapping when teams can’t swallow our recommendations. Reformulation, Winter, pp.24-27.
Concerning the Future of CAT and Other Relational Therapies
Dunn, M. and Dunn, S., 2012. Concerning the Future of CAT and Other Relational Therapies. Reformulation, Winter, pp.10-13.
Editorial
Lloyd, J. and Pollard, R., 2012. Editorial. Reformulation, Winter, pp.3-4.
Exploring whether the 6 Part Story Method is a valuable tool to identify victims of bullying in people with Down’s Syndrome
Pettit, A., 2012. Exploring whether the 6 Part Story Method is a valuable tool to identify victims of bullying in people with Down’s Syndrome. Reformulation, Winter, pp.28-34.
Letter from the Chair of ACAT
Hepple, J., 2012. Letter from the Chair of ACAT. Reformulation, Winter, p.5.
Past Hurts and Therapeutic Talent
Williams, B., 2012. Past Hurts and Therapeutic Talent. Reformulation, Winter, pp.39-42.
Reciprocal roles within the NHS
Welch, L., 2012. Reciprocal roles within the NHS. Reformulation, Winter, pp.14-18.
Relationships in Microcosm in Cognitive Analytic Therapy: Based on a workshop given at the 2012 ACAT Conference in Manchester
Hepple, J., 2012. Relationships in Microcosm in Cognitive Analytic Therapy: Based on a workshop given at the 2012 ACAT Conference in Manchester. Reformulation, Winter, pp.35-38.
The 16 + 1 interview
Wilde McCormick, L., 2012. The 16 + 1 interview. Reformulation, Winter, p.44.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.