Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.
The content of this paper arises from my work as a CAT practitioner and Clinical Psychologist working with individuals who engage in offending behaviours and the practitioners in mental health and criminal justice agencies surrounding these clients. The aim is to share clinical practice and use of CAT in working with individuals who are at risk of harming others, and to consider some of the processes, which may impact on gaining collaboration and contribution from clients around risk assessment. The aim is to invite comment and discussion around these important issues.
As CAT practitioners working with clients in a range of mental health settings, we are aware that not all individuals who offend or who are at risk of offending, are in receipt of services from the criminal justice, forensic or prison services. The experience of staff in local mental health teams highlights high caseloads, limited resource, complex clients with risky behaviours and for many, a lack of detailed, comprehensive, structured approach to risk management. The most extreme outcome of violence is of course homicide, which is relatively rare in comparison to other kinds of violence. However, in a the national confidential enquiry report Avoidable deaths, of those who were convicted of homicide and who had a diagnosis of mental illness, 74% of individuals were under the care of general psychiatric services with only 4 % under the care of forensic services, in the 12months before the offence. Professionals are increasingly required to assess the risks posed by clients (Ward & Eccleston, 2000) and to develop plans to aid the positive management of these risks. This may understandably raise uncertainty and anxiety for clinicians. In order to improve the practice of risk assessment and guide mental health staff, the Department of Health (2007) published guidelines for best practice in managing risk.
Of note for clinicians, the document highlighted that risk management was everybody’s business; it is seen as a required competence for all mental health staff. Safety was seen as being at the centre of all good health care. This was particularly notable for mental health work where there was recognition that this could be more challenging. (DOH, 2007). Risk is defined as the “nature, severity, imminence, frequency/duration and likelihood of harm to self or others. A hazard that is to be identified, measured and ultimately, prevented” (Is this where your quote closes?) (DOH, 2007) based on awareness of the importance and presence of certain conditions that are judged to be risk factors (Logan, 2006). Within this paper, the hazard is defined as the risk that the client is likely to pose to others.
The DOH managing risk guidance detailed 16 practice principles that should underpin best practice across all mental health settings. Some of these will be discussed within this paper, with a view to exploring how Cognitive Analytic Therapy (CAT) can contribute to risk assessment and risk management.
Best Practice Principles for Risk Management
Risk management should be conducted in the spirit of collaboration and based on a trusting relationship with the service user. It should build upon recognition of the service user’s strengths with an emphasis on recovery (DOH, 2007). These principles are in keeping with the ethos of psychological therapies, in general. However, CAT, with its emphasis on transparency and collaboration through the active use and sharing of CAT reformulatory tools--writing and mapping--is able to start the process of service users’ collaborative contribution to risk assessment on a firm footing.
The other principles highlighted for good practice recommend that risk assessment should take into account that risk can be general and specific, and that good management can aim to reduce risk and prevent harm. In addition, that where possible, all risks should be identified and formulations of the situations where the risks may occur, and actions to be taken by the practitioners identified (DOH, 2007).
CAT has the potential to meet these principles. CAT has, as its basic premise, the ethos of working alongside the client to develop an accurate, collaborative, relational reformulation; the process by which the client’s early or significant experiences have been internalised as reciprocal roles, with the development of unhelpful, intra-, interpersonal, and social patterns (Ryle, 1990). Reciprocal roles incorporate internalised beliefs, values, memories, emotions, roles, identity and status positions, and therefore, the expectations of the other. CAT is also “open to the sociological in the way that the mainstream of clinical psychology--or other therapies--are not” (Sutton & Gaskell, 2009, p. 6). CAT is explicit in its educative approach to aide reformulation, recognition and revision of unhelpful (Ryle and Kerr 2002) or, in the case of this paper, destructive and risk laden reciprocal role procedures (RRPs).
Cognitive Analytic Therapy’s Understanding of Complex Presentations
Individuals who are at greater likelihood of harming others are likely to have complex problems including narcissistic, antisocial and borderline personality disturbance (Reid and Thorne, 1997), such as outlined in the ‘broken egg’: an understanding of male aggression and violence (Shannon, 2002; Shannon, Willis and Potter, 2006). Individuals with such difficulties have typically experienced trauma, multiple disrupted attachments (Aitken and McDonnell, 2006), profound loss, deprivation and abuse (Aiyegbusi, 2004). Given such experiences, polarised and restricted reciprocal role repertoires can result, and the structure of the self becomes fragmented by partially or fully dissociated self-states (see Multiple Self States Model (MSSM, Ryle, xx). It is the process of dissociation, which is key to understanding and engaging people with complex presentations, including individuals who persistently engage in the harm of others. The understanding of dissociation is the underlying condition of all personality disorders (Bromberg, 1983).
Dissociation: A Key to Understanding Complexity and Difficulty to Evoke Change
Elizabeth Howell (2005) an American psychoanalyst and traumatologist specialises in the treatment of dissociative disorders. She incorporates CAT into her work, and her writings are invaluable in amplifying CAT’s understanding of personality disorder in relation to dissociation. In her book the Dissociative mind, Howells refers to Pizer’s (1998) description of the mechanism for dissociation “At severe levels of shock and discrepancy…paradox becomes bridgeable, and one deploys the default mechanism of dissociation. Here we recognise the essence of trauma: the disruption of the continuity of being (the illusion of being one self) (pp.141-142).
For individuals with traumatic childhood experiences and subsequent development of dissociative patterns, the absence of another to bear witness and to make meaning of these damaging experiences or neglect, remain unformulated, fragmented and therefore not integrated into the selves of the individual (Ryle and Kerr, 2002). As opposed to “We interact, and therefore I become” (Ryle and Kerr, 2002, p.59), for those with damaging experiences perhaps it is more like, if ‘we do not interact, I do not learn to interact with myself, or if I do it is by fractured and confused means’.
Howells (2005) also describes another process, not a default position of omission, but one of commission, of active dissociation. In a process outside of an individual’s awareness, vigilance and psychological resource are utilised by the individual in a desperate bid ‘not to notice’ and to ward off, traumatic memories and experience. Unattended perceptions and thoughts, loose their connection to other aspects of personal meaning and are therefore less likely to be recalled (Sullivan 1956). This process “begins with selective inattention and goes on to dissociation of events, with various degrees of awareness between” (Sullivan 1953, p63).
Whether the client’s early difficult experiences are unformulated or actively dissociated from, or perhaps both, the individual is unlikely to have a coherent understanding of themselves. These individuals are likely to have impoverished self-reflective, emotional identification and emotional expressiveness skills (Nathanson, 1994). This has direct implications for client’s ability to contribute to discussions surrounding risk of harming others.
Of course, the client may also be likely to be ambivalent to acknowledge their risky behaviour for fear of criminal justice response, judgement and shame. However, due to the nature of these aforementioned complex psychological difficulties, potentially coupled with their state of mind at the time of offence (Pollock, 2006), clients will not necessarily have a formulated understanding, or at times a clear account of their harmful patterns. If it is not relationally thinkable, it is not linkable (Howells, 2005) to risk laden reciprocal role procedures.
Current Approaches to Risk Assessment in Services
In forensic and other mental health services, clinicians can be uncertain, anxious and reluctant to gain the clients engagement and contribution to the risk assessment process. Therefore, despite recommendations to the contrary, it is commonplace for clinicians to engage in the process of risk assessment without contribution from their client. The clinicians therefore become solely reliant upon the use of risk assessment such as the structured clinical judgement (SCJ) risk assessment tools e.g. HCR20, assessment for risk of violence (see Webster, Douglas, Eaves & Hart, 1997) or RSVP (see Hart, Kropp & Laws), an assessment for risk of sexual violence. These risk assessment tools involve the practitioner making a judgement about risk of violence, based on combining, an assessment of clearly defined factors derived from research; clinical experience and knowledge of the service user; and the service user’s own view of their experience (DOH, 2007). SCJ approaches are recommended as good practice (DOH, 2007), however they can be completed without the contribution of the client, which often occurs.
When the client does not engage, hypotheses are generated to explain the client’s lack of contribution. It can be assumed that the client is ‘withholding’ of pertinent information, or aiming to ‘mislead’ or ‘manipulate’ the clinician and the systems surrounding the client. Whilst of course, this may be the case, given what we know about the complex psychological difficulties these clients experience and the psychological processes which are absent or employed, to protect the individual, this could be a reductionist perspective.
The client’s non-inclusion in the risk assessment processes is likely to contextually enact harmful reciprocal roles of control, neglect and exclusion. As long as staff/systems re-enact the client’s early object relations they contribute to the long-term psychopathology of the client (Dunn and Parry, 1997). The lack of contribution by the client also misses the opportunity for utilising the full benefits of using a relational, collaborative psychological model such as CAT. Which when employed, enhances engagement, increases understanding and motivation to engage in collaborative risk assessment and management.
Use of CAT to Motivate and Engage Client’s Contribution to the Risk Assessment Process
In the first instance, there is a process of negotiating engagement with the client who engages in behaviours, which pose a risk to others. Initially, the emphasis should be placed upon understanding, and exploration around the possibility for change. The focus is upon the joint curiosity and the process of making meaning with a reflective other, as opposed to initially recruiting the client to engage in change. This is in anticipation of the common contextual reciprocal role enactment of accusatory, powerfully imposing and controlling in relation to an imposed upon, judged and powerless individual. This is especially enacted within forensic systems (Aiyegbusi, 2004) and can be recognised, at times, as psychologically harmful (Walsh, 1996). The process of motivation and engagement should also be mindful of the client’s zone of proximal development (ZPD), (Vygotsky, 1978) and of course, non-collusion of pro-offending attitudes or behaviour.
Given that some individuals who engage in offending behaviour have impoverished or absent relationships the client’s experiences are “unsymbolised” and therefore unhelpfully enacted interpersonally. These experiences are not real or tangible unless they exist in a meaningful way, in the mind of the other (Howells, p106). Therefore the process of bearing witness and making meaning together with an empathic other, perhaps for the first time, are important early steps (Ryle and Kerr, 2002). Making links with these internalised early experiences with the development of current patterns of relating, including risky or offending procedures is the next step in reformulation.
The process of reformulation for individuals who are at risk of harming others, is to disentangle fantasy, fragmented memories, emerging risky behaviours and for some, preverbal experiences, to create as far possible, a meaningful narrative. This is a complex, yet necessary process to gain a reformulation and psychologically assist the individual to increase understanding regarding the origin(s) and nature of the risk. All of which can help form an accurate and detailed risk assessment.
CAT and Risk Assessment: Reciprocal Roles and Reciprocal Role Procedures as Specific Risk Patterns
Reciprocal Role procedures (RRP’s) are the fundamental unit of analysis and level of inference in CAT (Ryle, 1992). Within RRPs we can gain a collaborative description of intentional acts or enactments of roles in relation to others. It is by looking at the Reciprocal Role repertoire that we can begin to identify the relational nature of the client’s risk of harming others (Pollock, 2006). A fine detailed analysis of each RRP and associated self-state has the potential to provide relevant information required for general and specific risk assessment (as recommended in the DOH guidelines.)
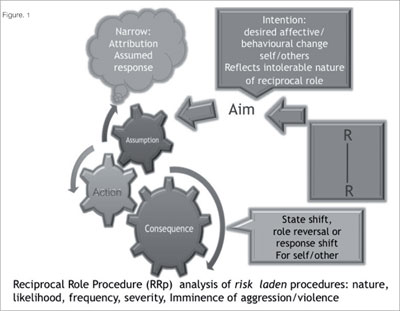
RRP’s are repetitive sequences of cognitive, behavioural, affective and interpersonal processes, which are rigid, unrevised, and therefore prevent change (Ryle and Kerr, 2002). RRP’s commence from a reciprocal role and have, in simple terms, the following components: aim, assumption or belief, behaviour and consequence. RRP’s provide a means of “formulating the offender’s motivations, intentions and probable reasons for the [offence]” (Pollock & Stowell-Smith, 2006, p.6). In working with an individual who has harmed another or who is at risk of doing so, the starting point is to determine the individual’s aim.
Usually the aim of a procedure is benign and reflects the intolerable states of mind from which the individual aims to find a solution e.g. ‘Aim to escape the pain’, ‘aim to feel better’ or ‘aim to find someone to be there for me.’ Establishing the individual’s aim forms the important role of empathising (Ryle and Kerr, 2002) and normalising the distress associated with the intolerable reciprocal role. The careful unveiling of the assumption within the individual’s ZPD provides the parameters and the assumed solution to meet the aim followed by the behaviour and the consequences of the action for self and others. With this client group, the action can be violence or aggression played out in reality and/or in fantasy.
From a risk assessment perspective, analysis of this procedure enables the client and therapist to understand the triggers, real or perceived, which position the client into the intolerable state of mind, and the likely courses of action which the client will take. Therefore the nature, the likelihood, severity and imminence of offending behaviour can be established (Hart, Kropp, Laws, 2003).
Figure 1.
Reducing Dissociation and Increasing Motivation for Reduction of Offending
With the collaborative development of a reformulation, the client can not only gain an understanding of the origins of their relational difficulties, but with support, the client can increase their awareness of the intolerable states of mind and associated procedures from which the risky behaviour is more likely to occur. Increased awareness and insight moves the offending behaviour from a partially dissociated self-state (emotions, memories, thoughts, behaviours, motivation) and therefore external to their sense of self, to a recognised and connected with state. With this shift, and level 3 understanding (see MSS model Ryle) there is the potential for this reciprocal role to be internalised and integrated fully within the selves of the individual. By the nature of this process, levels of dissociation are reduced i.e. naming, increasing recognition and making relational links. There is therefore an increased potential for the promotion of ownership and accountability for the risk posed to others. Quite often for some clients, this process elicits a new sense of empowerment, hope and choice to move toward creating non-offending exits from existing procedures and the possibility of effective risk reduction.
For some, this new self-understanding; recognition of responsibility and accountability for offending may be difficult and psychologically defended against. However, in my experience, the profound realisation of client’s control for their offending behaviour as being located within themselves; intra-personally, creates a powerful ‘ah ha’ moment which is difficult to defend or dissociate from. Moreover with continued support and reflection, the cognitive dissonance (Festinger, 1957) which this process evokes, makes it difficult for the individual to step back in time, to un-do the knowing of the intrapersonal origin of their offending behaviour. For example in an assessment, a young man’s RRP was recognised:
Feeling vulnerable and powerless, I aim to escape these feelings. I assume I must make some one else feel my pain, not me. I seek out an individual to goad, when they respond, that gives me the green light to attack him. So that it is he, not me, who is powerless, vulnerable, beaten. I am powerful and victorious.
The assessor recognised that the content of the assessment was likely to elicit an intolerable state of vulnerability, which may increase the likelihood of violence following the assessment.
By collaboratively sharing his RRP and helping the client generate some exits from his procedure, the risk potential was managed. The client had recognition of the procedure and, albeit begrudgingly, took account for his risk potential and followed his exit. The risk of violence was prevented on this occasion and was increasingly applied to other situations. CAT’s collaborative development of practical and realistic revisions to unhelpful procedures provides the new opportunity and practice of skills from which to learn to risk manage and reduce the likelihood of offending. Teaching clients to recognise and respond in high-risk situations as part of effective risk management is crucial (Dvoskin and Steadman, 1994)
Direct and Indirect Offending Procedures
The aforementioned was an example of a ‘direct’ offending procedure, that is, where there are rigid assumptions, behaviours and consequences, which contain aggression and violence. It seems where offending behaviour is pervasive in an individual’s experience; the repertoire of non-offending, healthy reciprocal roles and the RRP’s are minimal and there is little behavioural flexibility. Instead offending behaviours are utilised as intended solutions for relational conflict. By implication, this means that there may be a number of intolerable reciprocal roles with associated procedures, which have the potential to trigger violent or aggressive behaviour. For instance, the previous example of the young man, he had four self-states in his reformulation from which there was increased potential for violence.
Contrary to a frequent offender, not all clients offending behaviour is persistent or pervasive. For other clients there may be a broader repertoire of reciprocal roles, which include healthy reciprocal roles, and there may also be wider variation in the range of assumptions and behaviours for these ‘indirect’ offenders. For these individuals who offend, there does not appear to be an intentional offending act at the start of the RRP. Instead, it seems that it is the rigidity, tenacity and adherence to the aim and narrow procedure, which seems to ratchet up the behaviour and the consequences of this, spilling into the realms of offending.
For example, Tom chose to seek revenge for his perceived ill treatment and humiliation from an acquaintance. His assumption was that he could only avenge his mistreatment, by public humiliation. He perceived this would be a just and right punishment and provide some resolution to the incident for himself. However, after initial failed attempts, he was unable to revise his aim or his assumption and increased his attempts, in a desperate bid to achieve his aim. Tom began a process of entrapment in order to lure his acquaintance into offending and thereby humiliating him in the process. Tom was rigid in his adherence to his aim and assumption to the degree that he had little awareness that to continue this process and to ensnare his acquaintance, he himself had slipped into offending behaviour. When this came to the light of the police, he re-experienced intolerable feelings of humiliation and resentment. Tom had no prior pre-convictions, yet his aim to avenge his mistreatment ‘psychologically hijacked’ him and triggered an indirect offending procedure, when his aim was not initially realised. It was likely that Tom’s solution for feeling humiliated had always evoked antisocial behaviour, which was usually just within the margins of law breaking.
Using and Sharing Risk Reformulations
As discussed, the reformulation collaboratively identifies risk-laden RRP’s. The formulation will contain the nature, likelihood, imminence and the severity of the violence potential (DOH, 2007). Like all CAT reformulations this can be utilised by the client as a self-management tool. With the client’s recognition of their risk RRP’s, the clearly identified and defined exits can be employed earlier in the offending pattern. There is, therefore, a greater likelihood of preventing harm to others. The risk reformulation will also clearly identify the therapy needs of the client, which can form a coherent and relevant care plan aimed at both improving the psychological wellbeing of the client and public protection.
CAT’s strength is also as a systemic formulation (Ryle and Kerr, 2002). CAT practitioners can utilise the formulation to communicate a detailed understanding of risk procedures to staff, statutory and criminal justice agencies, and agree an informed, proportionate and collaboratively shared response. This is likely to be more effective and client, staff and multi-agencies are likely to have greater confidence in risk management plans.
Contextual reformulation also makes explicit the more complex processes involved in perpetuating and exacerbating an individual’s psychopathology which are implicit in the patient’s reformulation (Ryle and Kerr, 2002). Sharing the reformulation can also provide support and management of the anxiety for staff (Kerr, 1999; Ryle and Kerr, 2002). CAT offers informed ways of relating to the client, which do not enact early experiences (Dunn and Parry, 1997) and so do not perpetuate the client’s risk of violence.
Importantly, the CAT reformulation can also be incorporated into established, Internationally utilised and valued risk assessments (see HCR20 and RSVP) to provide a range of detailed, specific, effective risk management plans (scenarios) with shared agreement with the client and staff. A CAT informed risk management plan brings with it the added benefit of understanding the client’s intra-personal experience and its link with offending behaviour, and highlighting treatment needs and care plans.
“Clinicians who understand the importance of the setting and context, and their relationship to the internal vulnerability associated with different personality traits, will find it easier to recognize and assess risk and will be in a better position to help manage it” (Reid and Thorne, 2007 p.8). This paper has highlighted that CAT provides this, and has also demonstrated its ability to meet the DOH principles for good practice in risk management (DOH, 2007).
Summary
A CAT risk reformulation highlighting direct and indirect risk laden RRP’s can be incorporated into care plans and communicated to staff and agencies surrounding the client, whether we are CAT practitioners in forensic, adult, adolescent, learning disability or older adult mental health services. Given risk management is everybody’s business (DOH, 2007), as CAT practitioners we really can ‘use what we know’ to contribute to risk assessment, management and public protection.
Acknowledgements
I wish to thank Dr Dawn Bennett and Steve Potter for their helpful comments.
References
Aiyegbusi, A. (2004) Forensic Mental Health nursing: care with security in mind. Pfäfflin, F. and Adshead, G. A matter of security: the application of attachment theory to forensic . Jessica Kinglsey publishers. Uk.
Aitken, G. and McDonnell, K. The use of Cognitive Analytic Therapy with women in secure settings. In Pollock. P.H., Stowell-Smith. M. & Gopfert M. (Eds.). Cognitive Analytic Therapy for Offender: A New Approach to Forensic Psychotherapy. (pp. 295-314). Routledge.
Bromberg, P (1983) The mirror and the mask: On narcissism and psychonalaytical growth. Contemp. Psychoanal., 19:359-397. Department of Health. (2007) Best practice for managing risk.
Dunn, M. and Parry, G. (1997) A Reformulated Care Plan Approach to Caring for People with Borderline Personality Disorder in A Community Mental Health Service Setting. Clinical Psychology Forum 104 19-22.
Dvoskin, J.A. and Steadman, H.J. (1994) using intensive case management to reduce violence by mentally ill persons in the community. Hospital and Community and psychiatry July 1994 vol. 45, no.7
Festinger, L. (1957) A theory of cognitive dissonance, Stanford, CA: Stanford University Press
Hart, S.D., Kropp, R., & Laws, D.R. (2003). The Risk for Sexual Violence Protocol (RSVP). Mental Health, Law, and Policy Institute, Simon Fraser University.
Howells, E.F. (2005). The Dissociative mind. The analytic press, Inc., Publishers.
Kerr, I. B. (1999) Cognitive Analytic Therapy for Borderline Personality Disorder in the Context of a Community Mental Health Team: Individual and Organisational Psycho dynamic Implications British Journal of Psychotherapy 15(4) 425-437.
National confidential enquiry report Avoidable deaths, of those who were convicted of homicide and who had a diagnosis of mental illness,
Avoidable deaths: five year report of the national confidential inquiry into suicide and homicide by people with mental illness.
Logan, C., Structured Professional Judgement and Risk Formulation: Managing the Risk of Harm, paper presented at Mersey Care NHS Trust
Conference, November 2006.
Nathanson, R.W. (1994) Character styles. London. Norton Press.
Pizer, S. (1998) Building bridges: negotiating paradox in psychoanalysis. Hillsdale, NJ: The Analytic Press. In Howells, E.F. (2005). The Dissociative mind. The analytic press, Inc., Publishers.
Pollock. P.H (2006) The contribution of CAT to court proceedings. In Pollock. P.H., Stowell-Smith. M. & Gopfert M. (Eds.). Cognitive Analytic Therapy for Offender: A New Approach to Forensic Psychotherapy. (pp. 295-314). Routledge.
Pollock. P.H., Stowell-Smith, M. (2006) Cognitive Analytic Therapy applied to offending. In Pollock. P.H., Stowell-Smith. M. & Gopfert M. (Eds.). Cognitive Analytic Therapy for Offender: A New Approach to Forensic Psychotherapy. (pp. 295-314). Routledge.
Ryle, R., (1990) Cognitive analytic therapy: developments in theory and practice. Chichester: Wiley.
Ryle, A. and Kerr, I. B. Introducing Cognitive Analytic Therapy. Principles and Practice. Wiley: Chichester
Reid, W. H., & Thorne, S. A. (2007) Personality disorders and violence potential. Journal of psychiatric practice, 13 (4).
Shannon, K.L. (2002). Using CAT to understand aggressive men in forensic settings.Unpublished Essay. Submitted as part of CAT North practitioner training, Manchester.
Shannon, K.L. (2008) Using what we know: CAT and risk assessment. Paper presentation at CAT North conference: Innovations in clinical practice. Manchester.
Shannon, K.L., Willis. A., & Potter, S. (2006). Fragile states and fixed identities: using CAT to understand aggressive men in relational and societal terms. In Pollock. P.H., Stowell-Smith. M. & Gopfert M. (Eds.). Cognitive Analytic Therapy for Offender: A New Approach to Forensic Psychotherapy. (pp. 295-314). Routledge.
Sullivan, H.S. (1953) The interpersonal theory of psychiatry. New York: Norton.
Sutton, L & Gaskell, A. (2009) Meeting with older people as CAT practitioners” attending to neglect. Reformulation: theory and practice in cognitive analytic therapy. Issue 32 Summer 2009.
Vygotsky, L.S. (1978) Mind in society: the development of higher psychological processes. Cambridge, M.A.: Harvard University Press.
Ward, T., & Eccleston, L. (2000). The assessment of dangerous behaviour: Research and clinical issues. Behaviour Change, 17 (2), 53068.
Webster. C.D., Douglas, K.S., Eaves, D., & Hart, S.D. (1997). The HCR-20 Scheme: Assessing Risk for Violence (version 2). Simon Fraser University. Mental Health, Law and Policy Institute.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Helping service users understand and manage the risk: Are we part of the problem?
Crowther, S., 2014. Helping service users understand and manage the risk: Are we part of the problem?. Reformulation, Winter, pp.41-44.
Are we afraid to break tradition? Cognitive Analytic Therapy’s (CAT’s) contribution to the treatment of sexual risk
Sara Casado, 2018. Are we afraid to break tradition? Cognitive Analytic Therapy’s (CAT’s) contribution to the treatment of sexual risk. Reformulation, Winter, pp.26-31.
Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending
Mitzman, S. F., 2010. Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending. Reformulation, Summer, pp.26-30.
Developing a CAT understanding of Anti-Social Personality Disorder (ASPD)
Kerry Manson, Sunil Lad and Marisol Cavieres, 2017. Developing a CAT understanding of Anti-Social Personality Disorder (ASPD). Reformulation, Summer, pp.42-48.
The Clinician’s Guide To Forensic Music Therapy - Book Review
Wakeling, N, 2017. The Clinician’s Guide To Forensic Music Therapy - Book Review. Reformulation, Winter, pp.56-57.
Other Articles in the Same Issue
A Brief Survey of Perceptions of Cognitive Analytic Therapy Within Local Mental Health Systems
Turley, A., Faulkner, J., Tunbridge, V., Regan, C. and Knight, E., 2009. A Brief Survey of Perceptions of Cognitive Analytic Therapy Within Local Mental Health Systems. Reformulation, Winter, p.26.
A Call For Papers On The 3rd International ACAT Conference
Elia, I., 2009. A Call For Papers On The 3rd International ACAT Conference. Reformulation, Winter, p.25.
A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities
Wells, S., 2009. A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities. Reformulation, Winter, pp.21-23.
Chair’s Letter, October 2009
Westacott, M., 2009. Chair’s Letter, October 2009. Reformulation, Winter, p.3.
Cognitive Analytic Therapy, or Can You Make a Mad Man Sane?
Anonymous, 2009. Cognitive Analytic Therapy, or Can You Make a Mad Man Sane?. Reformulation, Winter, pp.11-13.
Darwin and Psychotherapy
Elia, I., 2009. Darwin and Psychotherapy. Reformulation, Winter, p.9.
Dialogue and Desire: Michael Bakhtin and the Linguistic Turn in Psychotherapy by Rachel Pollard
Hepple, J., 2009. Dialogue and Desire: Michael Bakhtin and the Linguistic Turn in Psychotherapy by Rachel Pollard. Reformulation, Winter, pp.10-11.
International ACAT Conference “What Constitutes a CAT Group Experience?â€
Anderson, N., M., 2009. International ACAT Conference “What Constitutes a CAT Group Experience?â€. Reformulation, Winter, pp.25-26.
IRRAPT 2007-9 Research Projects
McNeill, R., 2009. IRRAPT 2007-9 Research Projects. Reformulation, Winter, p.26.
K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples
Jenaway, A., 2009. K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples. Reformulation, Winter, pp.13-16.
Letter from the Editors
Elia, I., Jenaway, A., 2009. Letter from the Editors. Reformulation, Winter, p.3.
Letter to the Editors
Anonymous, 2009. Letter to the Editors. Reformulation, Winter, p.6.
Measurements of change and their relationship to each other in the course of a CAT therapy
Gallagher, G., Inge, T., McNeill, R., Pretorius, W., O’ Rourke, D. and Wrench, M., 2009. Measurements of change and their relationship to each other in the course of a CAT therapy. Reformulation, Winter, pp.27-28.
Recieving a CAT Reformulation Letter: What Makes a Good Experience?
Newell, A., Garrihy, A., Morgan, K., Raymond, C., and Gamble, H., 2009. Recieving a CAT Reformulation Letter: What Makes a Good Experience?. Reformulation, Winter, p.29.
Research Into the Use of CAT Rating Sheets
Coombes, J., Taylor, K. and Tristram, E., 2009. Research Into the Use of CAT Rating Sheets. Reformulation, Winter, pp.28-29.
The Big Debate - Health Professions Council
Jenaway, A., 2009. The Big Debate - Health Professions Council. Reformulation, Winter, p.7.
Threats to Clinical Psychology from the CBT Stranglehold
Lloyd, J., 2009. Threats to Clinical Psychology from the CBT Stranglehold. Reformulation, Winter, pp.8-9.
Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.
When Happy is not the Only Feeling: Implications for Accessing Psychological Therapy
Lloyd, J., 2009. When Happy is not the Only Feeling: Implications for Accessing Psychological Therapy. Reformulation, Winter, pp.24-25.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.