Using Cognitive Analytic Therapy with parents: some theory and a case report
Jenaway, A., 2007. Using Cognitive Analytic Therapy with parents: some theory and a case report. Reformulation, Winter, pp.12-15.
Dr Alison Jenaway
Introduction
Cognitive analytic therapy (CAT) is starting to be used in Child and Adolescent Mental Health (CAMH) services, where I work, as a consultant psychiatrist in psychotherapy, with young people who have emotional problems and relationship difficulties. There has also been one randomised controlled trial of CAT in 15 to 18 year olds with risk factors for borderline personality disorder, showing that it is better than treatment as usual for this group (Chanen, 2006).
I was interested to see whether the CAT model, and an SDR, could be helpful to parents of an adolescent who had relationship problems and acted out difficult reciprocal roles, even though the adolescent was not interested in therapy. It has been used in this way to offer consultation to mental health teams about difficult patients who are not willing to engage in psychotherapy themselves but are causing significant problems to the team or system that they are interacting with (Dunn and Parry 1997). This process is called Contextual Reformulation and the aim is to understand the reciprocal roles and difficult behaviour of a patient by consulting with those trying to help. A sequential diagrammatic reformulation (SDR) is created through discussing with team members how the patient makes them feel, and the sort of difficulties they get into when trying to help the patient. Often team members are split, with some being pulled into a very caring/rescuing role towards a “needy/helpless” patient, and others feeling angry and rejecting towards the “demanding/ manipulative” patient.
The unhelpful reciprocal roles are then identified on the diagram so that team members can start to recognise when they are being pulled into problematic roles and try to do something different. More helpful roles can be discussed and practiced so that the patient meets a more consistent “good enough” role whichever member of the team they are seeing. It is quite likely that parents and carers could also be split in this way, pulled into different reciprocal roles, or even the same one, but at different times. They may well end up arguing with each other about the best way to handle the child and the problems, rather than being able to present a more united (good enough) front and a more consistent approach.
A Developmental Model of Reciprocal Roles
Clearly when talking to a community mental health team, there is no suggestion that the staff have created the very roles they are finding so difficult to deal with, the origin of the roles is attributed to the past experiences and relationships of the patient. The standard description of the origin of reciprocal roles, which is that they are developed through the relationships that the child has with caregivers as it is growing up, is potentially much more threatening for parents. They may feel blamed and feel the need to defend themselves or their actions, and this can get in the way of trying to explain the model. Often parents can see that the problem roles are ones that they have learnt in childhood, but they had hoped not to pass on to the next generation. This can lead to very fruitful discussions of how as parents, we may try very hard to do the opposite of what our own parents did, but in the process cause similar problem roles. For those parents who are not so open to examining their own roles, or for those who have a child who seems biologically predisposed to problematic roles, I have found an explanation of reciprocal role development which was described to me by one of my trainees very useful. The model originated from Michael Knight and I have modified it a little so that it becomes a description of babies and how they develop. It makes it easier to talk about a variety of factors which may have led to problematic roles, rather than such a strong focus on parental interactions, and I think that makes it easier for parents to hear and take in with an open mind.
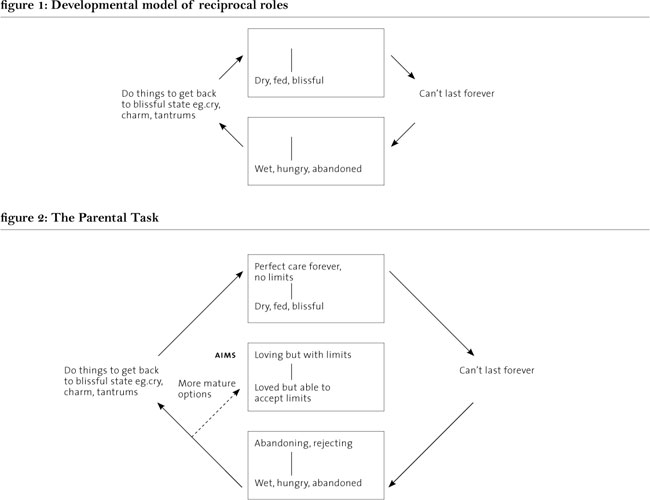
The model starts with the two extreme states of a baby, at the top of the diagram the baby is warm, fed, comfortable and blissful, all desires are fulï€lled. At the bottom the baby is hungry, wet and alone, feeling abandoned and rejected because the carer is not there immediately. On the left hand side are the procedures which the baby develops to try and get it’s needs met and get back up to the state of bliss – crying, being charming, temper tantrums etc. On the right hand side are the things which go wrong or interrupt the state of bliss (Fig 1). If parents can understand these states then it is fairly easy to add reciprocal roles to them and explain how our job as parents is to help the baby develop a middle ground area, where the baby can be upset at being hungry but still know it is loved and can learn to wait and be patient, and eventually to comfort itself.
The parents need to guide the infant on how to get it’s needs met in healthy, appropriate ways, rather than tantrums and demands (Fig 2). This model makes it easier to acknowledge that there are many factors which can interfere with this process, and that some of those are not under the parents’ control. There may be some babies who have inherited a temperament, or biological illnesses, which interfere with this learning process, even if the parental roles offered are good enough. Similarly, as in the case described below, early damage may have been done by initial carers, which is hard to repair even with good enough adoptive parenting later on.
The case
Kelly was a 15 year old, referred to the CAMH Service by the community paediatrician that she was seeing for her Chronic Fatigue Syndrome. She was doing well from this point of view but the family were still having difficulty managing her mood swings and her behaviour. Kelly was adopted into the family, with her younger sister Kate as babies. Kelly was 18 months old at adoption and Kate was adopted a couple of years later at 8 months old. They had the same biological mother but different fathers. Their mother had learning difficulties and made chaotic relationships with difficult men; she was unable to look after her children, in spite of support. Kelly’s father had a history of substance misuse. The children had always known about the adoption and could talk about it freely.
They had been seen as a family for family therapy 4 years earlier, but had found the sessions very difficult. The parents did not want to be critical of Kelly’s behaviour in front of her, and so it was hard to get to the bottom of the problems. Kelly was also referred for individual therapy from a fostering and adoption psychologist. This therapy focused on anger management and coming to terms with her adoption. On IQ testing her Full Scale IQ was 77 (Low). She had been seen by a consultant child and adolescent psychiatrist who did not feel that she was mentally ill.
I met with Kelly and her adoptive mum and the family therapist who already knew the family. Kelly was reluctant to talk and said very little. Mum explained that a few months before, Kelly had become very angry and aggressive towards Kate and said that she wanted to “put her in hospital”. Kelly had been sent off to stay with her adoptive grandparents for a few days to calm down. Mum was clearly desperate. She said that as parents they were just “surviving” and did not know how to cope. Nothing they did seemed to help or work.
Mum was reluctant to describe Kelly’s behaviour in front of her but said that sometimes she seemed very depressed, neglected herself and did not bother to wash or change her clothes. At these times, Mum almost had to look after her as if she was a baby. When asked about this Kelly was able to say that she could be happy and have fun out with her friends, but that she would like to be prettier and thinner like the members of the girl band “Girls Aloud”. If while they were out, anyone said anything which reminded her that she did not look like this, she would feel that there was no point in looking after herself at all and she would give up.
I started to try to draw a CAT diagram showing these different states but Kelly was not interested and did not want therapy. I decided to offer some sessions to Mum and Dad to see if using a CAT diagram could help them to understand and manage these mood swings and odd behaviour. Mum was sceptical that it could help but agreed to give it a go; we agreed to meet monthly for 3 sessions. The family therapist wanted to stay involved to observe CAT in action. The parents were also encouraged to attend a Triple P group for adoptive parents.
This is a group programme which helps parents understand and manage adolescent issues.
In the first session, the model above was explained to both mum and dad. It did seem to describe Kelly’s behaviour quite well. They described other states she could get into where she was “hyper” running around screaming and following her sister around stopping her going to bed. When they tried to set limits, she would often become rejecting and verbally abusive, threatening to destroy their possessions. She did not seem to care about them as parents or be attached to them, although she was close to Kate. We agreed that it might be possible to write down some exits, if they started to notice anything which worked and brought Kelly into the middle ground. They were encouraged to use the diagram to work out which states she was in over the next month.
At session 2, the parents had not used the diagram and had not noticed anything that had worked. They talked about how Kelly had stolen some money from mum and refused to give it back. Mum had been upset and furious and followed her, angrily, up to her room. Eventually, mum had given up and calmed down and Kelly had rolled over on her bed to reveal the money. Although mum and dad were adamant that Kelly never apologised or showed any remorse, we pointed out that she did, in her own way, show that she knew it had been wrong to steal and that mum being calm and backing off had worked. Mum seemed intensely upset by these behaviours and seemed to be pulled down into angry/rejecting to angry/rejected roles when they happened. Dad was a bit more resigned to the whole thing, but could still get angry at times.
Mum had tried to go to the Triple P group but found it all too much. She felt she could not go again as she would just be in floods of tears the whole time. We talked about the need to grieve for the daughter they didn’t have and start to accept the less than perfect one they did have. I asked them to think of things which they could say to themselves to help them stay in the middle of the diagram where I had written “caring, and calm, but with limits”.
At session 3, they had not thought of anything they could say to themselves and did not seem to have remembered the suggestion. I pointed out that they seemed to have been pulled down into the bottom of the diagram, having struggled for so many years. They seemed to feel hopeless and helpless and were desperate for someone to wave a magic wand as they did not feel capable of making any changes themselves. They agreed and said that it was so hard because things were so unpredictable, some days one thing would work but the next the same thing would not. We talked about the need to try and stay in the middle whether or not it “worked” in terms of changing Kelly’s behaviour, so that at least they could feel that they had managed things OK and could feel some self respect. For example, Dad said that he had given up expecting an apology after rude or abusive behaviour, because it was only given when she wanted him to do something and that it therefore was meaningless. I disagreed, I felt that for Kelly to apologise, even if she did not mean it, was important. Just to have to say the words meant that a part of her was giving in to the expectation that she and her parents should respect each other. It also meant that they could feel some self respect, rather than being left feeling abused and taken advantage of.
It still seemed impossible for them to come up with anything to write down as ways of staying in the middle. They reported that although they were not actively using the diagram, they had it in mind and the sessions were helping. We agreed a further 3 sessions.
At session 4, a shift seemed to have occurred. Instead of a list of terrible incidents, both parents talked about times when Kelly had actually surprised them with positive behaviour. Mum described that Kelly had refused to have the tetanus injection she needed. Mum had stayed calm and said “it’s up to you but you may not be able to work at the stables without it”. Kelly was keen to work with horses and she immediately agreed to have it. Mum also described how Kelly had called her an “old bitch” and then soon after had asked her mum for something. Mum had said “oh yes, the old bitch will do it” at which point Kelly said “oh I was angry with you, you know I didn’t mean it”. Although it was unorthodox, I felt that Mum had stayed calm and showed skilful use of humour as a way of saying that she was not taking it personally, but she was a bit upset. We managed to write some things down on our list at last:
- Point out the longterm consequences for her plans (rather than appealing to her to do something for your sake)
- Keep calm and make positive suggestions Mum and Dad also added:
- Remind ourselves that we have done our best and have done a good enough job with Kate.
- Accept that Kelly has to make her own choices now, even if she makes mistakes.
- Look after ourselves – recharge our own batteries.
- Remember that even normal teenagers are difficult.
We encouraged them to look at the list when things got difficult to remind themselves that they could find ways of staying in the middle and say more positive, encouraging things to themselves. They seemed more able to stand back from the behaviours and think about how to react.
At session 5, the whole atmosphere had changed, Mum and Dad seemed positive and happy. Although things were still really difficult they seemed to be coping. They said how helpful the thought of the diagram was in keeping them in the middle. It was also helpful to know that there was something wrong with the way she reacted and it was not all their fault. Neither could really remember any times when Kelly had gone into the strange “hyper” state. She had taken some responsibility to open her own bank account. Dad said that he was still waiting for an apology for some rude and abusive behaviour but that he would wait until Kelly wanted something and then he might get it. There did not seem much to talk about and we agreed to finish after these 5 sessions. They kindly gave me permission to write this case report.
The parents were asked at the last session to rate out of 10 on a visual analogue scale, how helpful the therapy had been (0= not at all helpful, 5=somewhat helpful, 10=extremely helpful). They both rated it as 9 out of 10. At three month follow up by telephone, Kelly’s mum said that although life was still not easy, they were taking each day as it came and no longer blaming themselves for all the difficulties. They were still using the diagram to keep in the middle and Kelly was doing well at her NVQ course. She wanted to say that, of all the therapies they had been offered, CAT had made the most sense.
Conclusion
Using Cognitive Analytic Therapy ideas and a diagram seemed to be helpful with this couple where systemic family therapy, individual therapy and a group programme for parents had been too hard for them, or had not been seen as very helpful. The diagram seemed to give them a greater understanding of what was wrong with Kelly. Although she had not been formally diagnosed as mentally ill, the diagram explained her personality difficulties so that they could see that there was something wrong with her and it was not all their fault. I think this allowed them to have more realistic expectations of both themselves and of Kelly so that the household became more relaxed and accepting. Rather than trying to control her behaviour (which always failed) the focus turned to them controlling their own behaviour (which was much more possible). We were able to gradually put into words what they needed to do to break the cycles they were stuck in with Kelly. This allowed them to experience some success, feel more in control, and regain their self esteem as parents. This, in turn, seemed to allow Kelly to start to meet them in the middle occasionally and to reduce some of her more extreme behaviours.
References
Chanen, A. et al (2006). A randomised controlled trial of psychotherapy for early intervention for borderline personality disorder. Acta Neuropsychiatrica, 18 (6) 319.
Dunn, M., Golynkina, K., Ryle, A., and Watson, J.P. (1997). A repeat audit of the cognitive analytic clinic at Guy’s Hospital. Psychiatric Bulletin, 21, 1-4.
Dunn, M. and Parry, G.D. (1997) A formulated care plan approach to caring for borderline personality disorder in a community health setting. Clinical Psychology Forum, 104, 19-22.
Ryle, A. and Golynkina, K. (2000) Effectiveness of time-limited cognitive analytic therapy of borderline personality disorder; Factors associated with outcome. British Journal of Medical Psychology, 73, 169-177.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Jenaway, A., 2007. Using Cognitive Analytic Therapy with parents: some theory and a case report. Reformulation, Winter, pp.12-15.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Change your Parenting for the Better - exploring CAT as a parenting intervention
Dr Alison Jenaway, 2013. Change your Parenting for the Better - exploring CAT as a parenting intervention. Reformulation, Winter, p.32,33,34,35,36.
Using a template to draw diagrams in Cognitive Analytic Therapy
Jenaway, Dr. A. and Rattigan, N., 2011. Using a template to draw diagrams in Cognitive Analytic Therapy. Reformulation, Summer, pp.46-48.
Service Innovation
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.
What Happens After “Happy Ever After�
Jenaway, A., 2010. What Happens After “Happy Ever After�. Reformulation, Summer, pp.8-9.
K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples
Jenaway, A., 2009. K.I.S.S. (Keep It Simple. Stupid) - Reflections on Using CAT with Adolescents and a Couple of Case Examples. Reformulation, Winter, pp.13-16.
Other Articles in the Same Issue
A Sign for the Therapeutic Relationship
Akande, R., 2007. A Sign for the Therapeutic Relationship. Reformulation, Winter, pp.6-7.
Cuckoo Lane
Elia, I., 2007. Cuckoo Lane. Reformulation, Winter, pp.4-5.
Evidence submitted by the British Association for Counselling and Psychotherapy (NICE 92)
Rowland, N., 2007. Evidence submitted by the British Association for Counselling and Psychotherapy (NICE 92). Reformulation, Winter, p.20.
In the Beginning was the Conversation 'Process' Spirituality and CAT
Dunn, M., 2007. In the Beginning was the Conversation 'Process' Spirituality and CAT. Reformulation, Winter, pp.16-19.
Letter from the Editors
Elia, I., Jenaway, A., 2007. Letter from the Editors. Reformulation, Winter, p.3.
States Characterisation Procedure (SCP) for supporting the reformulation of patients with borderline/dissociative features
Ryle, A., 2007. States Characterisation Procedure (SCP) for supporting the reformulation of patients with borderline/dissociative features. Reformulation, Winter, pp.9-11.
Using Cognitive Analytic Therapy with parents: some theory and a case report
Jenaway, A., 2007. Using Cognitive Analytic Therapy with parents: some theory and a case report. Reformulation, Winter, pp.12-15.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.