Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group
Psaila, C.L. and Crowley, V., 2006. Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group. Reformulation, Winter, pp.5-11.
The following article originally appeared in a longer form in Mental Health and Learning Disabilities. The reference is: Psaila CL & Crowley V (2005) Cognitive Analytic Therapy in People with Learning Disabilities: An investigation into the common Reciprocal Roles found within this client group. Mental Health and Learning Disabilities: Research and Practice. 2(2), 96 – 108.
Introduction
Development of psychotherapy for people with learning disabilities
Historically it was thought that people with learning disabilities would not benefit from psychotherapy (Tyson & Sandler, 1971). Until the last two decades, most published therapeutic research for people with learning disabilities was either behavioural or medical. Development of psychotherapy with people with learning disabilities was intricately tied to political and societal changes in the fundamental treatment and understanding of people with learning disabilities. Lack of evaluation of effective outpatient treatment for people with learning disabilities is one of the underlying reasons why people with learning disabilities are often excluded from psychotherapy (Nezu and Nezu, 1994).
Psychoanalysis for people with learning disabilities
It is now recognised that people with learning disabilities do benefit from psychotherapy. Sinason (1992) states that patients with profound disabilities can benefit from psychoanalytic psychotherapy because communication takes place on more than one level. She distinguishes between cognitive and emotional intelligence: ‘emotional intelligence may be left intact and rich regardless of how crippled performance intelligence was’. Human contact at a fundamental emotional level can be made with most people. This in itself may be therapeutic. Thereafter, practitioners should adjust and apply their skills to the presenting problem in a way that can be usefully accepted (Decker, 1988). Bates (1992) regarded working with people with learning disabilities psychotherapeutically to differ from working with non-handicapped people only through the process having a different time span and rhythm.
‘At a fundamental level, working with a person with a learning disability in psychotherapy is the same as working with anyone else, and as different. They are often not seen as suitable for treatment, but here it is psychotherapy that is handicapped.’ Linington (2002)
Using Cognitive Behaviour Therapy (CBT) with people with learning disabilities
Previously the behaviour of people with learning disabilities was considered objectively but without regarding meaning. This ignoring of the person’s motivation led to labelling their wish for human contact in a negative way (Lovett, 1985). CBT with people with learning disabilities enables the therapist to bring into awareness the motivation driving the behaviour. CBT therapists aim to make the relationship collaborative, regarding issues of social control and who sets the therapy goals (Kroese et al 1997).
Kroese et al (1997) illustrated in their seminal book, that people with learning disabilities were able to work within the structure of CBT, which offered these clients some control over their therapy, a real choice, and an opportunity to express themselves. The researchers found that clients engaged in CBT were more likely to listen, take psychological concepts on board and work in a collaborative way than clients who did not receive CBT. This demonstration of people with learning disabilities working effectively within, and understanding the concepts of a CBT framework has paved the way for the use of other therapies such as Cognitive Analytic Therapy (CAT).
Psychotherapeutic issues
Hollins & Sinason (2000) suggested a number of psychic organising principles, which have to be dealt with in psychotherapy for people with learning disabilities:
• The existence of the disability. Including conscious and unconscious fantasies that accompany it. The existence of disability at birth impacts on the relationship of the individual with their family and community (Hollins & Sinason 2000). There is an increase in emotional disturbance in proportion to the severity of the learning disability (Szivos & Griffiths, 1990).
• Issues of loss of the normal self who would have been born.
• Dependency, including the problems of not being able to live autonomously. This may make it more difficult for disabled teenagers to take the first steps towards adult life.
• Sexuality, which may be distorted by the impact of the disability. People with learning disabilities may receive contradictory messages about their sexuality and the appropriateness or inappropriateness of their behaviour (Sigman 1985). Limited spoken language skills may hinder communication about the emotional feelings of emerging sexuality, sexual experience, or abuse.
• Fear of death or murder, including being part of a group that society wishes to eliminate e.g. foetal screening. Smiling and withdrawing may be different responses to this fear. This is impacted by exclusion from more concrete aspects of death and death rituals.
Other related themes
Some other related themes discussed in the literature are briefly outlined below:
- Attachment. From birth, the parents’ overwhelming grief and unresolved mourning impact on care giving and the development of a secure sense of self (Ainsworth & Eichberg, 1991; Bowlby 1979). Hollins & Sinason (2000) consider that where there is disruption to bonding as a result of the disability, the disability itself is experienced as a trauma.
- Trauma. Some experiences of disability may result in trauma. Hollins & Sinason (2000) considered that ‘traumatic symptoms are significantly under-recognised in people with learning disabilities’. One aspect of this may be illustrated by the ‘handicapped smile’, formulated by Sinason (1992) as a function of appeasement rather than happiness. This reaction may develop as a result of fear towards an aggressor.
- Secondary handicap. Secondary handicap, or the exaggeration of the learning difficulty, may give the person with learning disability some control over it, thus making it less unbearable. Stokes & Sinason (1992) said ‘we feel with nearly all our clients there is an extra potential not being fulfilled’. They found it useful to distinguish between two states that people move in and out of, one in which the handicap is predominant and another in which a more perceptive and less damaged self is predominant. This possibility depends on severity and organicity.
Effect on therapist/community
Psychotherapy is about “the mutual experience of handicap”. (Linington, 2002). Disabled individuals can represent damaged aspects of the self that people want to be rid of, realised by a wish to hide people with disabilities away from the community. Someone’s particular disability may reveal to another the emotionally powerful aspects of their own early models of recognition and negation. Bender (1993) spoke about the therapeutic disdain towards people with learning disabilities and the attitudes of mental health professionals towards clients with learning disabilities.
Cognitive Analytic Therapy (CAT) with people with learning disabilities
Crowley (2002) has shown that people with learning disabilities are able to utilise and understand the model of CAT (see Ryle 2002, p.173). It is well suited for use with people with learning disabilities. It incorporates Vygotsky’s (1978) idea that what a child is allowed to do with the support of another influences what it learns to do independently, and so the therapy may act to compensate for some of the emotional interactions missed in childhood. CAT may aid self-reflection, which is a skill people develop as they go through life; and an increase in self-reflection could improve cognitive capacity. CAT is explicitly collaborative and respectful. It uses clear descriptions with pictures and diagrams, which may enable people with learning disabilities to learn more equal ways of relating to others, addressing issues of dependency and powerlessness. CAT has also been useful in enabling staff groups to recognise the Reciprocal Roles (RRs) of some of the clients, helping them to avoid collusion with client’s maladaptive RRs.
The lack of full cognitive and verbal abilities means that people with learning disabilities are limited in their responses and ability to cope (for example, with their parents’ grief or rejection; or with abuse or ostracism). They have lacked the opportunity and ability to develop effective coping strategies. This may result in someone with learning disabilities being unheard or misunderstood.
In a relationship with a psychotherapist, people with learning disabilities may feel overwhelmed and be unable to express worries about sexual feelings or thoughts about such feelings toward the therapist. They may experience the therapist as rejecting/abandoning unless termination is well addressed. Alternatively, they may idealise the therapeutic relationship. Idealised RRs may lead to a belief that fulfilment of these roles will make them perfect or perfectly cared for. A therapist could collude with these by giving special care, rescue or protection, leading to inevitable disappointment. Collusion also dis-empowers and de-skills the client. It does not help them prepare for everyday disappointments in life or allow them to come to terms with their learning disability and real lives, or to acknowledge what they do have.
The CAT model provides a forum for exploration of these issues. It examines the client’s relationships with others and with the therapist, through an understanding of the client’s RRs. Ryle (2002) cited common RRs within this client group, as being Abusing or Bully to Abused or Victim, Not Hearing or Understanding to Not Heard or Understood, Rejecting to Rejected and Abandoning to Abandoned. These RRs were identified through clinical judgement rather than research.
Aim
Having worked within a department where CAT was used to work with clients with learning disabilities, the opportunity arose to conduct research into the Reciprocal Roles (RRs) of people with learning disabilities. Identification of RRs is important so the therapist does not collude with the client and reinforce unhelpful patterns.
The aims of this research were 1. to formally acknowledge common RRs observed in working with people with learning disabilities, confirming the RRs identified in Ryle (2002); and 2. to explore how these roles may link to common psychotherapeutic issues.
Method
Design
In this exploratory investigation to identify common RRs for people with learning disabilities, an empirical methodology was employed which involved gathering of data and induction of patterns (Coolican, 1990). The qualitative data was analysed using content analysis and is presented using descriptive statistics.
Participants
Clinical judgement was employed to decide whether CAT would be an appropriate approach for each routine referral to a psychological service for learning disabilities. The therapists were qualified or trainee clinical psychologists, or nurse behaviour specialists, all receiving regular supervision for their cases from a qualified CAT therapist. The participants for the research were chosen using criterion sampling (Miles & Huberman, 1994), i.e. all cases in the department which had been seen for CAT therapy were used. There were sixteen appropriate cases. Each of these was housed either in the community or in forensic services. There were 11 male participants: 5 in the community and 6 in forensic. There were 5 female participants: 4 in the community, 1 in forensic.
Procedure and data analysis
Each participant had twenty to twenty-four sessions of CAT. The reformulation letters, psychotherapy files, sequential diagrammatic reformulation, therapy notes, and goodbye letters of each participant were collated. For reasons of confidentiality each participant’s notes were given a case number, which was used as a reference throughout the therapy records. The records were systematically scrutinised for RRs.
Content analysis (Krippendorf, 1980) was used to analyse the data. This involved initially sampling the data and then coding it:
Sampling – Each piece of data was examined for RRs. These were extracted from the original data in order to be coded.
Coding – the data was then structured and coded in two stages:
- Stage 1: Indigenous categories – the data was coded with wording used by participants.
- Stage 2: Researchers’ categories – the data was then coded further using categories identified by the researchers.
Some RRs were more challenging to code than others, e.g. some RRs contained a number of different words and thus may have been appropriate for different categories. It was decided by the researchers to code these RRs according to the overall meaning.
Repetition of the research cycle and Triangulation
These procedures were done to increase the credibility of the results. Repetition of the research cycle means that the raw data was revisited to check and re-check earlier assumptions and inferences made. Two methods of Triangulation were used: 1. different records were examined for each participant, and 2. two different researchers coded the data.
Self reflection of researchers
Qualitative research is vulnerable to researcher bias. Some of the RRs were difficult to categorise, particularly the roles that were abstract or had many parts to them. In these cases they were coded by meaning for the first researcher. The first researcher was independent of the therapy. This was an advantage in the sense that she could be more objective about the data, but a disadvantage with regards to having a true understanding of the nature of each RR. The second researcher also coded the RRs. She was involved in the therapy of all the participants, either as a therapist or as a supervisor and therefore understood the implicit meanings of all the RRs.
Results
Overall results
Twenty-two different RRs were identified, including four ideal RRs: ‘rescuing/caring — rescued/cared for’; ‘special/ perfect — learning disabled’; ‘admiring — admired’; ‘in control — fragile’. Overall, the sixteen participants identified eightythree RRs, twenty of which were ideal RRs. There was an average of 5.1 RRs per participant, ranging was between 3 and 8 RRs per participant.
Fifteen of the RRs were identified by more than 10% of participants. The most common were ‘abusing — abused’; ‘rejecting — rejected’; ‘rescuing, caring for — rescued, cared for’; ‘damaging — damaged’; ‘abandoning — abandoned’; ‘special, perfect — learning disabled’;
Forensic and community results
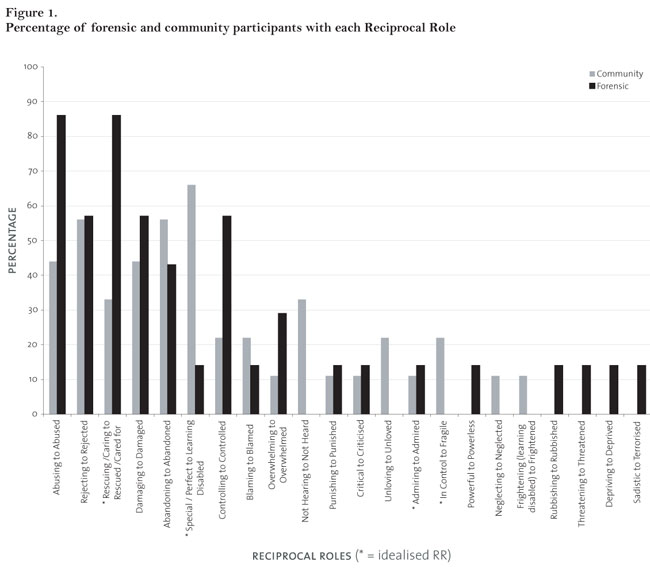
Whilst analysing the data, differences between community and forensic participants were noted. Figure 1 shows how the RRs were distributed between forensic and community participants.
It can be seen from the graph that three of the most commonly identified RRs are found fairly evenly in both the community and forensic population.
- • ‘Rejecting — Rejected’ 56% in the community and 57% in forensic
- • ‘Damaging — Damaged’ 44% in community and 57% in forensic
- • ‘Abandoning — Abandoned’ 56% in community and 43% in forensic
Forensic
Seventeen RRs were identified within the forensic participants, seven of which were identified in 29% to 86% of the forensic participants; the other ten in less than 15% of them.
From Figure 1 it can be seen that the majority of forensic participants, 86%, had ‘abusing — abused’, compared to 44 % of participants in the community. There were also more forensic participants with the ideal RR ‘rescuing/caring — rescued/ cared for’ 86% compared to 33% in the community. ‘Controlling — controlled’ was over twice as prevalent in forensic services (57%) as in the community (22%).
Community
Seventeen RRs were also identified in community participants, eleven of which were identified in 22% to 66% of the participants; the other six in less than 12% of them.
The graph shows that there were some RRs that were identified mainly in the community population. The RRs ‘not hearing — not heard’, ‘in control — fragile’, and ‘unloving v unloved’ were identified in 33%, 22%, and 22% of community participants, respectively, but none of these RRs was identified in forensic participants. The ideal RR ‘Special/ Perfect — Learning Disabled’ was over four times more prevalent in the community population, where it was identified in 66% of the participants, compared to 14% in the forensic participants.
Discussion
The aim of this study was to identify common RRs for people with learning disabilities. Four common RRs for people with learning disabilities were identified:
- Abusing or Bully—Abused or Victim
- Damaging—Damaged
- Rejecting—Rejected
- Abandoning—Abandoned
Two idealised Reciprocal Roles were identified: • Rescuing/Caring—Rescued/Cared for
- Special/Perfect—Learning Disabled.
Ryle (2002) had previously identified a similar list of common RRs, except that ‘damaging-damaged’ was not included, and ‘not hearing or understanding—not heard or understood’ was. In this study, the RR ‘not hearing or understanding--not heard or understood’ was equally or less frequently identified compared to the following three RRs:
- Controlling—Controlled
- Blaming—Blamed
- Overwhelming—Overwhelmed
Further investigation is needed to determine whether these RRs are common enough to be included as a generalisation.
There was greater variation in the presentation for forensic participants with the RR ‘damaging—damaged’. The language used by forensic participants felt raw and hard-hitting; words like ‘destroyed’ and ‘terminator’ were used, expressing how damaging and damaged these participants felt. Further investigation into the significance of this role (and the closely allied ‘rejecting—rejected’) may be warranted, as both were identified in 57% of the learning disabled forensic participants.
There were more occurrences of the RR ‘abandoning— abandoned’ in the community. Three of the participants used the words ‘blanked off ’ or ‘cut off ’ in this RR. This reflects their response to being abandoned. Blanking off is a coping mechanism employed to protect the self from the experience of being abandoned, rather than being overwhelmed.
The ideal RRs reflect a fantasy or idealised projection of a relationship. The ideal RR’s listed here may be understood as a reaction to some of the psychological issues highlighted in the introduction by Hollins & Sinason 2000 and others. One example of this would be the experience of a disability as a trauma, particularly if it causes a disruption to attachment (see p4 and 5). These concepts seem to be reflected in the ideal reciprocal role ‘Special/Perfect—Learning disabled’. A person may understandably fantasise about being special/perfect as a reaction to a learning disability, which may be traumatic and have caused additional psychological insults in addition to every day challenges. This was the second most frequent RR and found in 44% of the cases.
Another psychotherapeutic issue for people with learning disabilities, according to Hollins & Sinason (2000), is dependency. This may have been reflected in the RR ‘rescuing/ caring—rescued/cared for’, as it was the most frequent ideal RR, identified in 56% of all participants and identified more than twice as often in forensic participants. Being rescued/ideally cared for may also be a fantasy reaction to disrupted attachment processes.
The issues of emerging sexuality and sexual abuse may have been expressed through the RRs ‘abusing--abused’ and ‘damaging—damaged’. Because of their limited language skills, therapy is for many people with learning disabilities the first time that they have been helped to express their thoughts about sexual feelings and discuss memories of traumatic sexual events.
Attachment issues for people with learning disabilities have been discussed by a number of people (see Linington, 2002). The RRs ‘overwhelming—overwhelmed’ and ‘unloving— unloved’ may reflect attachment difficulty. The graph above shows that the majority of participants with ‘Overwhelming to Overwhelmed’ were in the forensic service, but all the participants with ‘unloving—unloved’ were in the community. These two RRs may be addressing similar issues from different perspectives.
Attitudes of mental health professionals towards people with learning disabilities (Bender, 1993) may reinforce the ‘rejecting--rejected’. Any RR may be played out between the therapist and client, particularly ‘not hearing—not heard’, ‘rubbishing—rubbished’ or ‘blaming—blamed. Reyes-Simpson (2004) discusses the challenging nature of therapy for both the therapist and client with learning disabilities. It is important that the therapist does not reinforce any of the RRs in therapy, although the identification of them can be a useful therapeutic tool. It is important to address these issues in supervision.
People with learning disabilities seem to have fewer RRs than people without learning disabilities. This may be influenced by dependence on other people and services, and may reflect not having a strong sense of self. Also, fewer roles are identified or can be worked on throughout the duration of therapy. This observation may be linked to Ryle’s (1999) observation that people who have experienced trauma have a restricted repertoire of RRs. A formal comparison of the numbers of RRs between people with and without learning disabilities could prove this.
Sigman (1985) and Cohen’s (1986) ideas that some people with learning disabilities cling to an immature way of being may impact on how a person with learning disabilities relates to their RRs. This may differ from working with other client groups. During the analysis of the therapy scripts it was noted that in some cases the therapist helped the client to recognise a more and less able self in order to do therapy with the more able self as described by Stokes & Sinason (1992).
The sample size of this research was small, partly due to the qualitative nature of the investigation and partly to using criterion sampling. Criterion sampling may have led to sample bias for two reasons:
- It was not recorded why these particular participants underwent CAT therapy. A more overt record of why each participant had CAT therapy and why others did not would have been informative.
- All the participants were treated by clinicians from the same learning disabilities service
The size was sufficient for a small pilot investigation, but a larger and more diverse sample would increase the external validity and generalisability.
Research into the RRs of people with learning disabilities who are not referred to psychological services would give a more general idea of common RRs in this client group. Hollins and Sinason (2000) suggest that increased emotional disturbance is a function of learning disability. It would therefore be interesting to see which RRs are related specifically to having a learning disability, as opposed to mental health problems. This could be done by comparing RRs of people with learning disabilities with the RRs of their non learning disabled peers –highlighting which RRs were specifically due to having a learning disability.
Conclusions
This study addressed the research aim by identifying common Reciprocal Roles for people with learning disabilities. Although not generalisable to all people with learning disabilities in psychological services, by increasing the research knowledge base, these results are useful for CAT therapists working with people with learning disabilities. This research formally endorses the common RRs initially suggested by Ryle (2002). It may also be useful for other clinicians considering the use of CAT or any other psychotherapy with people with learning disabilities. Awareness of these findings should help therapists avoid colluding with unhelpful RRs. Further research has been suggested to find out more about RRs with people with learning disabilities. Clinicians must take care not to assume RRs, to listen to the client, and to use their words.
CL Psaila & V Crowley
Acknowledgements
We would like to acknowledge and thank Jackie Wells, Jackie Drohan and Dr Nicola Murphy for their contributions to this research.
References
Ainsworth, M; Eichberg, C. 1991. ‘Effects on infant-mother attachment of mother’s unresolved loss of an attachment figure, or other traumatic experience’. In Murray Parkes, C; Stevenson-Hinde, J; Marris, P. (Eds.) Attachment Across the Life Cycle. London, Routledge.
Bates, R. 1992. ‘Psychotherapy with people with learning disabilities’. In: Waitman, A Conboy-Hill, S. (Eds.) Psychotherapy and Mental Handicap London, Sage.
Bender, M. 1993. ‘The unoffered chair: the history of therapeutic disdain towards people with a learning difficulty’. Clinical Psychology Forum 54: 7-12. Bowlby, J. 1979. The Making and Breaking of Affectional Bonds. London, Routledge.
Coolican, H. 1990. Research Methods and Statistics in Psychology. London, Hodder & Stoughton. Cohen, S. 1986. ‘Sense of defect’. Journal of the American Psychoanalytical Association 34: 47-56.
Crowley, V. 2002. p173 in Ryle, A. Introducing Cognitive Analytic Therapy: Principles and Practice. Chichester: Wiley.
Decker, R.1988. Effective Psychotherapy. New York, Hemisphere Publications.
Hollins, S; Sinason, V. 2000. ‘Psychotherapy, learning disabilities and trauma: new perspectives’. British Journal of Psychiatry 176: 32-36.
Krippendorf, K. 1980. Content Analysis: An Introduction to its Methodology. Beverly Hills, CA, Sage.
Kroese, B; Dagnan, D; Loumidia, K. (Eds.) 1997. Cognitive Behaviour Therapy for People with Learning Disabilities. London, Routledge.
Linington, M. 2002. ‘‘Whose Handicap?’ Psychotherapy with people with learning disabilities’. British Journal of Psychotherapy 18 (3): 409-414. Lovett, H. 1985. Cognitive Counselling and Persons with Special Needs. New York, Praeger.
Miles, M; Huberman, A. 1994. Qualitative data analysis. London, Sage.
Nezu, C; Nezu, A. 1994. Outpatient Psychotherapy for Adults with Mental Retardation and Concomitant Psychopathology: Research and Clinical Imperatives. Journal of Consulting and Clinical Psychology 62 1: 34-42.
Reyes-Simpson, E. (2004). When there is too much to take in: Some factors that restrict the capacity to think. In Simpson, D; Miller, L. Unexpected gains: Psychotherapy with people with learning disabilities. Karnac Books, London, p122-132.
Ryle, A. 1999. Cognitive Analytic Therapy and Borderline Personality Disorder: The Model and the Method. Chichester, Wiley.
Ryle, A. 2002. Introducing Cognitive Analytic Therapy: Principles and Practice. Chichester, Wiley.
Sigman, M. 1985. Individual and group psychotherapy with mentally retarded adolescents. In Sigman, M. (Ed.) Children with Emotional disorders and Developmental Disabilities: Assessment and Treatment. (pp. 259-277). New York: Grune & Stratton.
Sinason, V. 1992. Mental Handicap and The Human Condition: New Approaches from the Tavistock. Free Association Books, London.
Stokes, J; Sinason, V. 1992. Secondary Mental Handicap as a defence. In Waitman, A; Conboy-Hill, S. (Eds.) Psychotherapy and Mental Handicap. Sage Publications, London.
Szivos, S.E; Griffiths, E. 1990. Group processes involved in coming to terms with a mentally retarded identity. Mental Retardation 28: 333-41.
Tyson, R.L; Sandler, J. 1971. Problems in the selection of patients for psychoanalysis: comments on the application of ‘indications’, ‘suitability’ and ‘analysability’. British Journal of Medical Psychology 44: 211-28.
Vygotsky, L.S. (1978). Mind in Society: The Development of Higher Psychological Process. Cambridge MA, Harvard University Press.
Full Reference
Psaila, C.L. and Crowley, V., 2006. Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group. Reformulation, Winter, pp.5-11.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities
Wells, S., 2009. A Qualitative Study of Cognitive Analytic Therapy as Experienced by Clients with Learning Disabilities. Reformulation, Winter, pp.21-23.
The Inner Voice Check
Elia, I., 2007. The Inner Voice Check. Reformulation, Summer, pp.28-29.
Relational patterns amongst staff in an NHS Community Team
Staunton, G. Lloyd, J. Potter, S., 2015. Relational patterns amongst staff in an NHS Community Team. Reformulation, Summer, pp.38-44.
Exploring whether the 6 Part Story Method is a valuable tool to identify victims of bullying in people with Down’s Syndrome
Pettit, A., 2012. Exploring whether the 6 Part Story Method is a valuable tool to identify victims of bullying in people with Down’s Syndrome. Reformulation, Winter, pp.28-34.
Editorial
Lloyd, J., and Pollard, R., 2014. Editorial. Reformulation, Summer, pp.3-4.
Other Articles in the Same Issue
Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group
Psaila, C.L. and Crowley, V., 2006. Cognitive Analytic Therapy in People with Learning Disabilities: an Investigation into the Common Reciprocal Roles Found Within this Client Group. Reformulation, Winter, pp.5-11.
Developing a Language for the Psychotherapy of Later Life
Hepple, J., 2006. Developing a Language for the Psychotherapy of Later Life. Reformulation, Winter, pp.23-28.
Letter from the Chair
Mary Dunn, 2006. Letter from the Chair. Reformulation, Winter, p.4.
Letter from the Editors
Irene Elia and Alison Jenaway, 2006. Letter from the Editors. Reformulation, Winter, p.2.
Musings on Doing CAT with Couples
Gray, M., 2006. Musings on Doing CAT with Couples. Reformulation, Winter, pp.29-31.
Reflections on the Second International CAT Conference Maynooth, Ireland 15 - 17 June 2006
Donald Bermingham, 2006. Reflections on the Second International CAT Conference Maynooth, Ireland 15 - 17 June 2006. Reformulation, Winter, p.22.
Updating the Psycho-Social Checklist
Pollard, R. and Toye, J., 2006. Updating the Psycho-Social Checklist. Reformulation, Winter, pp.19-21.
'Don't Dis' Me!' using CAT with Young People who have Physical and Learning Disabilities
Collins, S., 2006. 'Don't Dis' Me!' using CAT with Young People who have Physical and Learning Disabilities. Reformulation, Winter, pp.13-15.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.