CAT and Eating Disorders
Harvey, L., 1994. CAT and Eating Disorders. Reformulation, ACAT News Spring, p.x.
Eating disordered clients can be assumed to be as diverse as others in their presentation and symptomatology, so it is worth reminding ourselves of the criteria for assessing patients for CAT.
“CAT is a safe first intervention for any not hopelessly substance-abusing patient, unless symptomatic issues are too powerful or fragmentation too extreme” (Ryle 1993).
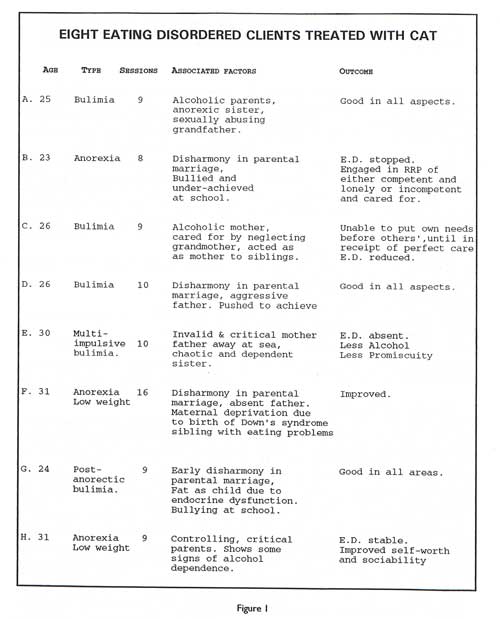
Eating disorders encompass a broad range of symptoms. They may be seen as a progression from “simple” anorexia nervosa of childhood onset, to bulimia with anorectic tendencies. The latter may be “simple” or unimpulsive bulimia nervosa or multi-impulsive bulimia, which has marked similarities to borderline personality disorders. Multi-impulsive bulimia has been much discussed by Professor Hubert Lacey (see figure 2 below).
Although I have no personal experience of treating obese binge eaters, I would suggest that they might find CAT as beneficial as anorexics and bulimics. Fairburm and Wilson (1993) suggest Interpersonal Therapy (IPT) or Cognitive-Behavioural Therapy (CBT) as treatments for severe binge eating. Where dietary problems predominate, CBT is used first; if it fails IPT is tried next. Where interpersonal problems predominate, IPT is used first; if it fails, CBT is tried next. I believe that CAT bridges the gap between IPT and CBT quite effectively, and could show as good as, or even better, rates of success than these separate therapies, with greater economy of time and other resources, if the therapists are sufficiently experienced.
However, experience is not all and CAT also provides a holding structure, when as a therapist one is floundering in the face of a barrage of counter-transference and armour-plating that has thickened with age.
Jeanne Magagna (1993) asks, “Does the therapist have the willingness and capacity to meet the needs of a child who has not yet transformed bodily experiences into emotions suitable for language to be used in therapy: for example the silent, negative or borderline child.”
She describes the stance of such patients as:
I. Don’t touch.
2.You’re useless.
3. I want you to understand without my having to speak
4. Can you allow me to be separate?
I make no apology for relating the adult behaviour to the childhood presentation as in many cases the adult client presents in a very similar way.
Often the necessity for reformulation when no information has been given by the patient offers an opportunity to feed back to her the experience of her behaviour. The interpretations based on it often open the door to either confirmation and elaboration, or elucidation. There is no need to impose interpretations onto the client It is more a question of offering them as a starting point.
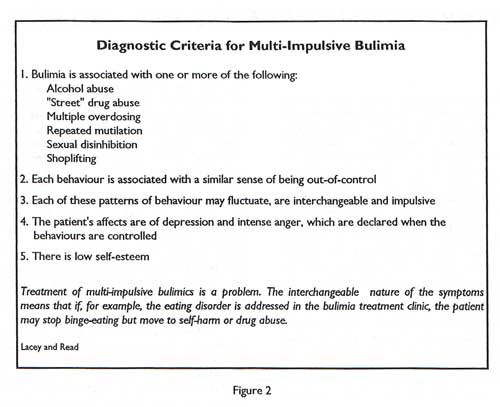
It has been my experience that the outcome of the therapies I have undertaken has been more satisfactory as I have gained experience and more background knowledge in the treatment of the disorder. Figure 1 is a review of eight cases treated by me, not listed in chronological order of treatment.
References
Fairburn, CG & Wilson, GT (1993) (eds) Binge Eating: Nature Assessment and Treatment, Guildford Press.
Lacey JH & Read TRC (1993) Multi-impulsive Bulimia: An Inpatient Eclectic Treatment Programmem in Eating Disorders Review, Wiley.
Magagna, J (1993) Individual Psychodynamic Psychotherapy in Childhood Onset Anorexia Nervosa and related Eating Disorders, Lask B, & Bryant-Waugh R (eds), Erlbaum Assoc.
Ryle, T (1993) “
Tony Ryle Briefly Interviewed By Mark Dunn
” ACATnews, vol2.
Linda Harvey
Full Reference
Harvey, L., 1994. CAT and Eating Disorders. Reformulation, ACAT News Spring, p.x.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice
Wicksteed, Dr. A., 2012. Using a Cognitive Analytic Therapy approach in working with Eating Disorders: Reflections on Practice. Reformulation, Summer, pp.26-31.
CAT Effectiveness: A Summary
Quraishi, M., 2009. CAT Effectiveness: A Summary. Reformulation, Summer, pp.36-38.
A Little Italian Story – Service Development
Fiorani, C., Poggioli, M., 2009. A Little Italian Story – Service Development. Reformulation, Summer, pp.13-14.
Perfectly Imperfect: Reflections of a Newly Qualified Clinical Psychologist in using CAT to Explore the Relational Contribution to Binge Eating
Dr Lyndsey Holt, 2017. Perfectly Imperfect: Reflections of a Newly Qualified Clinical Psychologist in using CAT to Explore the Relational Contribution to Binge Eating. Reformulation, Winter, pp.28-32.
A Call For Papers On The 3rd International ACAT Conference
Elia, I., 2009. A Call For Papers On The 3rd International ACAT Conference. Reformulation, Winter, p.25.
Other Articles in the Same Issue
Adult Survivors of Childhood Sexual Abuse : A Discussion of Definitions, Prevalence, Incidence and Theory as it applies to CAT Practice
Tanner, C., 1994. Adult Survivors of Childhood Sexual Abuse : A Discussion of Definitions, Prevalence, Incidence and Theory as it applies to CAT Practice. Reformulation, ACAT News Spring, p.x.
CAT and Eating Disorders
Harvey, L., 1994. CAT and Eating Disorders. Reformulation, ACAT News Spring, p.x.
Supervision: Integrating Self and Skill
Welch, L., 1994. Supervision: Integrating Self and Skill. Reformulation, ACAT News Spring, p.x.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.