Applying Cognitive Analytic Therapy to Guide Indirect Working
Carradice, A., 2004. Applying Cognitive Analytic Therapy to Guide Indirect Working. Reformulation, Autumn, pp.18-23.
A Case Study Describing Group Staff Consultation to Help Care Planning for a Client in the Inpatient Service
Abstract
Cognitive Analytic Therapy (CAT) was initially developed as a psychotherapy for use directly with clients. Over time there have been developments in applying CAT indirectly with staff to help them in their work with clients. This paper summarises the literature describing the use of CAT reformulation in indirect work. The value of using CAT Reformulation indirectly is illustrated by a case study of consultation with a staff group struggling with a challenging client in an inpatient service.
A. Introduction
Cognitive Analytic Therapy (CAT) developed by Tony Ryle, is a collaborative time-limited psychotherapy which involves developing a reformulation of how early experiences influenced the development of unhelpful patterns which maintain current difficult experiences. The reformulation is usually represented in a letter and a diagram or sequential diagrammatic reformulation (SDR). CAT was developed initially for working directly with clients. However, over time there has been work to apply CAT to indirect working. Indirect work involves assessment, formulation and interventions designed to impact positively on clients (Nicholson and Carradice, 2002). For example, working with staff to help support them in using psychological approaches in their role. This includes consultation, supervision and training. This paper summarises the literature on the use of CAT indirectly and describes a case study using CAT reformulation to inform team consultation and care planning for work with a challenging client in the inpatient setting to illustrate this indirect work. The setting for the case study provides 24-hour care for people with severe and enduring mental health problems. The clients mainly have a diagnosis of psychosis and have been in hospital for most of their lives. It is a continuing care setting, where most residents will live for the rest of their lives. The focus of the service is to provide intensive support to achieve and maintain the highest quality of life possible, whilst minimising the impact of relapse in mental ill health. The clients experience frequent psychotic relapses and between relapses they cope with a high level of residual positive and negative symptoms, such as hearing voices, experiencing delusions and poor motivation. Their social functioning has been severely compromised by repeated psychotic episodes and their experiences in institutions.
B. Descriptions in the Literature of Indirect Applications of CAT Reformulation
There is a growing literature describing the use of CAT principles, including CAT reformulation, when working indirectly; to aid understanding of psychologically harmful work environments (Walsh, 1996); Contextual Reformulation (Ryle and Kerr 2002a,b); with people with borderline personality disorder (Dunn and Parry, 1997; Kerr, 1999) and Learning Disability services (Lloyd and Williams, 2003). Each publication offers insight into the use of CAT principles indirectly, the value of doing so and future development. Each of these areas will be considered in turn:
i. The Process of Using CAT Principles Indirectly
There is diversity in the literature about how CAT is used in this type of work. However the principles of CAT to guide the development of the working relationship with the staff and/or clients are followed, including; being proactive, with an emphasis on active participation; agency (Ryle and Kerr, 2002a); being collaborative (Ryle and Kerr, 2002a,b) and developing diagrammatic and narrative CAT reformulation (Walsh, 1996; Dunn and Parry, 1997; Kerr, 1999; Ryle and Kerr 2002a,b). The literature describes working only with the staff team (e.g. Walsh, 1996) or working with the client and the staff team (e.g. Dunn and Parry, 1997). In the case of Dunn and Parry (1997) they describe a process whereby the clinician assesses the client directly for 3-4 sessions pulling together a reformulation of the client’s early life and the procedures which are maintaining their problems. The clinician then uses a reformulation letter and diagram developed with the client, to share understanding with the staff team and to inform the care plan. In other cases, the client may be unable to engage in this process because they are too stuck or too ill or the client may believe that they do not have a problem (Ryle and Kerr, 2002b). Then the mapping out of the diagram, including the reciprocal role enactments, can be constructed on the basis of discussion with the staff and/or family involved (Ryle and Kerr, 2002b). As well as discussion with others or assessment with the client, the Walsh (1996) example illustrated the value of direct observation by the clinician to inform understanding, as part of a research process also involving qualitative interviews with staff.
The literature describes the development of SDRs with the client during indirect work in the same way as followed in individual psychotherapy (for example, Dunn and Parry, 1997). However there are also developments from this towards simple contextual reformulation (e.g. ‘Brenda’ in Ryle and Kerr, 2002b) and extended (or more complex) contextual reformulation (e.g. Walsh, 1996; Kerr, 1999; Ryle and Kerr, 2002b). A contextual reformulation involves describing and mapping the responses of staff and in the more complex reformulation a number of other agencies may be involved (Kerr, 1999). The contextual reformulation makes explicit the more complex processes involved in perpetuating and exacerbating the individual psychopathology which are implicit in the patient’s reformulation (Ryle and Kerr, 2002b).
The publications illustrate how these reformulations are used to help work on exits, either with the staff or with both staff and patient. For example, with the staff team Walsh (1996) was able to help them openly discuss, own and develop exits to the organisational diagrammatic reformulation.
ii. The Value of Using CAT Reformulation in Indirect Work
The descriptions in the literature illustrate the value of using CAT reformulation when working indirectly. Benefits are clearly seen for patients (e.g. Ryle and Kerr, 2002b) and staff (e.g. Walsh, 1996). For example, when staff teams are working with difficult clients, they rarely have adequate resources such as time, training, supervision and the skills (Kerr, 1999). As a result staff teams can become collusive in their reactions to a client, and they describe them as ‘attention seeking’, ‘acting out’, ‘behavioural’, ‘bad, not ill’ (Dunn and Parry, 1997). In these circumstances there is the potential to result in staff splitting (Ryle and Kerr, 2002b). There is often high expressed emotion surrounding the client and staff are enacting different role reactions, either reciprocating or identifying with counter transference role enactments that serve to maintain the unhelpful procedures. The team contribute to the long-term pathology, as long as they ‘blindly’ reenact early object relations (Dunn and Parry, 1997). For example, in the case of Andrew (Ryle and Kerr, 2002a), much of his psychotic behaviour was, in the clinician’s view, essentially enactments of comprehensible but maladaptive attempts of coping with the illness. However, his behaviour was worsened by attempts of staff and family to ‘force’ treatment and react with hostility to his ‘noncompliance’. When working in this way, the team can split. For example, some members may have empathy for a patient and may over-identify with them, leading to being drawn into striving to provide the special care, which is unachievable. Others may react to behaviour by the client in punitive ways. The staff may then disagree on the approaches to use. These processes result in stress, reduced staff morale and burnout (Ryle and Kerr, 2002b). Whilst such enactments occur, the patient is not being best served by the team.
The value of CAT reformulation is that the difficulties are located in the system (Ryle and Kerr, 2002b). The difficulties and counter transference reactions can be transformed into collaboratively worked on and understood reactions (Ryle and Kerr, 2002b). This is helpful for staff and the patient (Ryle and Kerr, 2002b). The understanding can serve to give a sense of the patient’s distress within a framework of their past and present (Ryle and Kerr, 2002a), increase empathy for patients (Ryle and Kerr, 2002b) and show both the staff and patient that someone is listening (which can lead to better working relationships). CAT provides a concrete, nonjudgmental, visually accessible, coherent, engaging and understandable model to make sense of the previously powerful and confusing behaviours and feelings (which previously may have been experienced as dangerous (Walsh, 1996)). As well as understanding for staff, (which can be a relief (Walsh, 1996)), the reformulation then provides support and containment of the anxiety for staff (Kerr, 1999; Ryle and Kerr, 2002b). The negative reactions can then be owned and discussed openly (Ryle and Kerr, 2002b). Kerr (1999) describes how reformulation can help provide the ‘secure base’ for staff to work with disturbed patients. This understanding can then help work on exits; for example to create, strengthen or mobilise the therapeutic power of the relationship between the patient and those working with them (Ryle and Kerr, 2002b), and to plan interventions and keep working on them. The reformulation will predict transference and counter transference reactions, (Dunn and Parry, 1997) thereby helping staff with self awareness and reflection. Without the reformulation, all interventions are likely to involve re-enactment of the early object relations (Dunn and Parry, 1997). The reformulation can help staff respond helpfully, rather than collusively (Ryle and Kerr, 2002b).
iii. Areas for Development in Using CAT Indirectly
The literature published so far demonstrates the value of CAT in working indirectly. Overall the use of reformulation has been diverse and clinicians aim to provide reformulation in a way that suits the context of the work. A good reformulation is one that is useful (Kerr, 1999). Dawson (1988) described the intention that with disturbed clients the staff team can aim at least to ‘do no harm’. CAT reformulation provides a tool to help with this. However, the work published so far is case by case and naturalistic. It would be beneficial for further controlled evaluation of the potential efficacy to be carried out (Kerr, 1999; Ryle and Kerr, 2002a; see Walsh, (1996) for discussion of the complexities of this).
C. Group Staff Consultation to Help Care Planning for a Client in the Inpatient Service
The Case Example: Brief Summary
i. Referral
During a weekly multidisciplinary (MDT) meeting, several support workers (unqualified staff) demonstrated that they were feeling frightened of and demoralised by working with one particular client. During the discussion they requested a consultation session with myself as the psychologist in the team. A time was set for later that day.
ii. The Client
Jack, who is 57, has been hospitalised since he was a teenager. His index offence was injuring someone with a knife whilst experiencing an acute psychotic episode. He spent a large part of his life in a high security mental hospital, being transferred to 24-hour residential care on a Section of the Mental Health Act in the 1980s.
Throughout the years Jack has consistently displayed challenging behaviour including violence to staff, property and other clients, verbal aggression, intimidatory behaviour and high anxiety. He is preoccupied with his physical health, his positive psychotic symptoms and the staff attention towards him. He also experiences poor motivation, lethargy, poor social skills and a lack of interest in activities. These could be described as negative symptoms of psychosis, results of institutionalisation and compromised social functioning caused by repeated psychotic relapses.
Jack rarely engages in therapeutic activity on the unit and fears going out (so he rarely does). He will engage in basic self-care and assists with a couple of chores each day. He spends most of his time sitting, drinking tea and smoking. He will have conversations with staff about his experiences in the secure hospital, his body and physical health and will talk in ways that appear psychotic. He struggles to talk about other subjects and has poor self awareness.
iii. Assessment : Consultation With The Staff Group
During the meeting with staff in the afternoon there was a high level of distress and expressed emotion in the team (support workers, Named Nurse and OT). My role was to listen, be empathic and contain their distress. Staff were describing feeling angry towards Jack and being punitive towards him. They were also describing feeling frightened, victimised and unsafe. Some staff had both experiences with Jack. They were demanding that ‘something must be done’ because the staff team felt ‘uncared for’ and ‘alone’. They justified how bad it was by talking of how ‘even Jack’ kept apologising to them for his behaviour. As they ventilated their feelings, they became more able to talk about patterns. They described putting a big effort in to Jack, but it always came back to aggression. They also said he was ‘attention seeking’ and how difficult it was to manage this. Other patterns involved Jack suddenly becoming aggressive and threatening violence. Their responses were either to confront him by being just as confrontational and aggressive which tended to escalate things, or they felt frightened and abused, until someone stepped in and they were able to escape. Whilst the team were able to talk in patterns, I asked questions such as ‘what happens then?’, ‘how do you feel then?’ whilst drawing patterns on a sheet of paper with them. I checked out the patterns with the staff as I drew them.
At the end of the session the team reported that they felt calmer and more able to think clearly. However, they wanted help to decide what to do. We agreed to use the information they had provided to inform a team planning away day to pull together everyone’s experience and develop a care plan to guide what they did with Jack.
iv. Understanding the Context: The Staff Team
The inpatient service has four units totaling 34 beds and is staffed by 70. This large staff group has experienced a history of poor management, few resources, little (if any) training and limited clinical supervision. The staff group often felt disempowered and distressed at work. These factors combined to account for the provision of poor care and negative practice with residents. In recent years there have been increased resources and improved management. This has included influencing the staff experience of work positively by the provision of extensive training, support, clinical supervision for all staff and providing a psychological perspective to the management of the staff. These interventions have influenced the internal resources of staff sufficiently to enable them to begin to work collaboratively on using psychological approaches to their work. Previously, work to improve understanding and approaches used with residents were unsuccessful. This was because staff were unable or unwilling to see a need for change (precontemplation stage of change, Prochaska and DiClemente, 1986). The interventions that aimed to improve staff experiences of work served to support movement to a stage of change where they were more ready to generate, listen to and consider alternative ways of working.
v. Reformulation
I met with the Named Nurse and OT for three planning sessions to develop a programme for the away day. We used the information gathered during the earlier consultation to develop a reformulation and plan for an educational component for the away day to help with the team developing the care plan. In collaboration with the nurse and OT we developed a draft SDR for Jack.
|
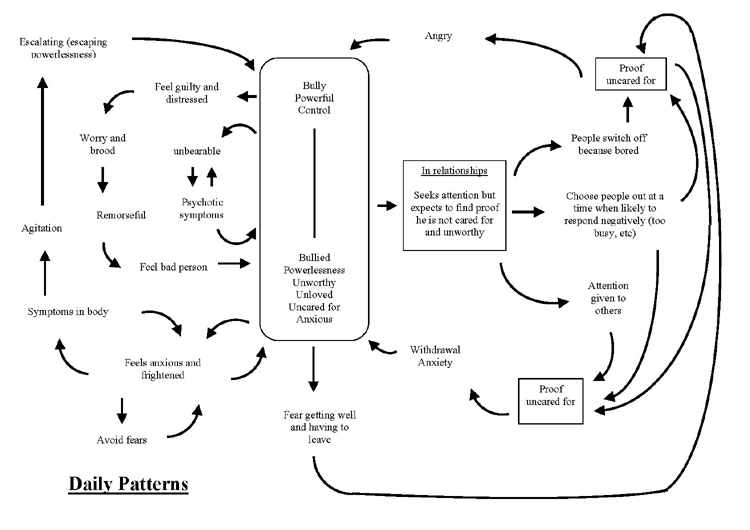
Table Two: Explanation of SDR The SDR illustrates a reciprocal role ‘bully, powerful and controlling’ to ‘bullied, powerless, unworthy, uncared for, unloved and anxious’. On the right of the diagram patterns illustrate that his child derived experience fuels a procedure where Jack fears getting well and having to leave hospital because that would be proof that he is uncared for, making him angry and enact the bully role. Another procedure is where Jack seeks attention to feel cared for (but expects he will find proof he is not cared for). He then talks to people in ways that bores them, proving he’s uncared for, making him angry and bullying or he talks to people when they are busy, which leads either to anger and bullying or to anxiety and re-experiencing the powerless, unloved, unworthy child role. He also tries to get attention, but sees attention going elsewhere to another client. He sees this as proof he’s uncared for again leading him to anger and bullying or anxiety and powerlessness. On the left of the SDR additional procedures have been drawn. Firstly from the child derived role Jack feelings of anxiety and fear escalate as he tries to avoid his fears. He then becomes preoccupied with the bodily sensations which increases into agitation and then enacts the parent derived role to bully others. From this experience he feels guilty, he worries and broods, feels remorse and apologises to others, feeling like a bad person. This confirms the child derived experience. In a sense he’s bullied himself into feeling unworthy and powerless. Jack also escapes, when all becomes unbearable, into psychosis where his madness takes over. Another example of self to self enactment is when Jack describes his experiences in the high security hospital where he was bullied, powerless and unworthy. Whilst he continues to be preoccupied with talking about this, he continues to repeat the experience.
Examples of Staff Experiences |
Alongside the draft SDR we drew a draft procedure which had staff reactions on it highlighting a particularly difficult repeating pattern.
|
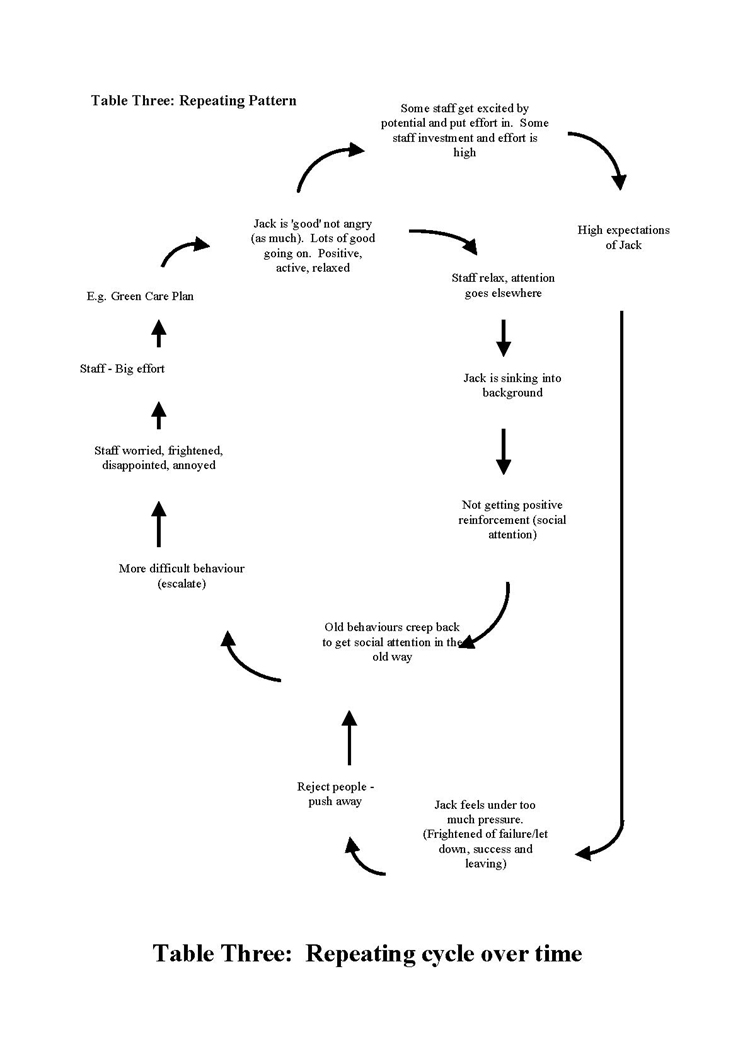
Table Four: Repeating Procedure and Explanation This procedure describes what happens for Jack and the staff. It begins with things going well for Jack making the staff relax and focus their efforts elsewhere. Jack feels that he’s sinking into the background and is missing positive social interaction. This results in Jack’s negative feelings surfacing and increased challenging behaviour. As the behaviour escalates, staff become distressed, angry and frightened. They put in a huge effort to try and change things for Jack and eventually his behaviour improves. The cycle then repeats itself. In addition, some staff are drawn into striving to provide special effort for Jack and have high expectations of him. This creates pressure and he feels anxious and pushes staff away, the challenging behaviour escalates and the pattern described previously takes over. |
Over a period of about a month, the nurse spent time observing Jack and the team to consider whether these two diagrams seemed accurate and useful or not. The nurse reported back after this observation that the reformulation seemed helpful.
The next stage was planning the team ‘day out’ where everyone could contribute to help with the development of the care plan. To do so we prepared exercises to help them ventilate and explore their reactions to and feelings about Jack. We also aimed to offer support, containment and help people develop understanding of the CAT principles and reformulation. This was intended to facilitate development of self awareness of their reactions and to discuss them openly in order to free the discussion about how to work on exits including a different relationship with Jack which was not collusive.
vi. Brief Summary of the Content of the Away Day: Team Planning Day For Jack
Together we developed a schedule for the day which involved five sections:
1. Emotional Reactions and Experiences
This involved helping staff to ventilate and then normalising their reactions and feelings.
2. Making sense
Describing and then encouraging discussion of the repeating pattern (Table Three).
3. Education about CAT principles including object relations and reciprocal roles
4. Jack’s SDR (Table One Above).
This section involved describing the SDR, getting feedback on it and then supporting staff to give examples of Jack following procedures or showing role enactments. Next we supported them to look at their reactions and put them on the map. This was done as a guided self discovery to ensure that we moved at their pace and worked where their understanding and self reflection was at.
5. Exits
This section involved discussion and education around having a different relationship with Jack, coping with feelings, education on anxiety and anger management approaches to the symptoms of these emotions. We also planned to review the principles of green care planning1 and develop ideas with the team to help write the new green care plan.
We developed specific exercises to help involve the staff in the educational components: eg. about anxiety and its management.
vii. The Away Day (The Process)
The day was attended by all 17 staff working with Jack and we followed the planned schedule described above. Initially the staff appeared tense and a little anxious about being at the away day and seemed to be experiencing high expressed emotion. The first exercise allowed them to ventilate and express these feelings in a nonjudgmental atmosphere. This then allowed them to open up and think more clearly. The rest of the day was collaborative, involving open discussion, honesty, debate and agreement over the plans for working with Jack. Outlining the repeating procedural pattern (Table Three) and the SDR was inspiring for staff and they reported new insights. Staff were fascinated by CAT principles and accepted the ideas as they had validity to them. The team had ownership in the development of the care plan and everyone contributed ideas. The away day was full of staff enthusiasm, motivation was high and staff reported during the feedback that the day had helped them understand their feelings and reactions and they felt freed to work differently with Jack. There was also feedback from the team that they felt valued and listened to during the process.
viii. Hypotheses About Change and Outcomes
When staff have no training or little theoretical knowledge to work with people with extreme behaviour, they have few resources to inform their understanding. Without theoretical understanding their cognitive appraisals about the behaviour of the client become personalised. For example ‘they do it to get at me’, ‘they don’t appreciate what I do’, ‘how dare they do that’. Such appraisals burn down the empathy that they feel for the client and it becomes increasingly difficult to work with them. Emotional or intuitive reactions guide what staff do with clients in such circumstances and, particularly when there is poor self awareness, reciprocal role enactments are played out blindly. Intervening to provide alternative appraisals that are theoretically (rather than personally) driven help the staff regain their empathy and there are possibilities for improved care.
It is difficult to measure outcomes from such an intervention with staff. However, there did seem to be changes in how the staff team worked with Jack. For example, in the weekly MDT meetings staff referred to the new green care plan and reported fewer incidents with Jack. Staff described him in less emotive terms and were able to discuss his progress. The nurse is in the ideal position to monitor progress and he continued to support staff in the daily handover and supervision to help them stay focussed on the approach. During the Care Programme Approach (CPA)2 Review meeting a couple of months later the nurse reported continued progress with Jack. Staff reported few incidents and were developing their relationship with him. Over the next few months other changes were reported - Jack became less anxious, began to attend his tribunals and CPA meetings (previously unknown), he began to take trips out more frequently (for example, going swimming) and started college. He appears happier some of the time and more able to talk about different topics to the old favourites. At eight months since the day out the informal feedback is that it was a worthwhile piece of work.
D. Discussion and Conclusions
This case study draws on the literature about using CAT principles and specifically diagrammatic reformulation with a staff team to help inform care planning.
i. Follow up
The most difficult stage in implementing any change is maintenance. I expect that the staff will require a follow-up or booster session to remind them of the reformulation, which I plan to provide when necessary.
ii. Lessons and Reflections
The case study describes using CAT to inform indirect working. The intervention impacted positively on the staff empathy level and provided alternative cognitive appraisals for their experiences. SDRs provide something useful to staff without training in how to understand clients’ distress and their own reactions. The approach was accessible to the support workers who have limited ability to self-reflect. CAT was containing for the clinician, helping to maintain neutrality when in the centre of expressed emotion and thereby preventing enactment of unhelpful patterns with the staff.
The original intention was to work with the team on the basis of trying to change their ways of relating to avoid collusion and maintenance of Jack’s unhelpful procedures (to do no harm, Dawson, 1988). However, in this case it seems as though there was more benefit for Jack than that, with the positive reports of his progress. The value of the green care plan is that it helps operationalise how to develop a positive relationship with the client as well as providing specific goals to work on. This supports the exits from SDRs and helps staff work on internalising the approach that works with the client.
iii. Critical Appraisal
This case study was limited by time resources causing a lack of formal evaluation to demonstrate changes such as records of frequency of adaptive and challenging behaviour. The work could have also been improved by collaborative involvement of Jack, the client. However, this was not possible (as described in Ryle and Kerr, 2002a,b) since Jack is unable to talk about his early life, or engage in conversations about his behaviour or experiences. Attempts to talk to him about such subjects result in anxiety, aggression and mental health relapse. In practical terms it was helpful for the staff, and therefore for Jack, to continue without his involvement (rather than not do the work at all). One cost, however, is that the SDR may be missing important information as it is based on observation, staff reactions and imagination. The potential for positive change justifies the work (especially since the ‘problem’ is located in the system, rather than the client).
In addition it may be that the SDR could have had a reciprocal role about emotional deprivation (emotionally depriving to deprived and unloved) which may have more sensibly driven some of the procedures about wanting attention and care. However, again the intention was to work with the information that came from the discussion. Another criticism could be that the repeating procedure may have been better included on the SDR, rather than the separate sheet, to make the origins clearer. However, the two diagrams were judged against the criteria that a good reformulation is one that is useful (Kerr, 1999). Working where the staff were at is important and they could identify the repeating procedure and their role in it, but the other enactments needed to be generated by self discovery in the teaching session. It may be that over time a more accurate SDR could be created and that Jack becomes more able to participate in conversations about his experiences and patterns.
Acknowledgements
I wish to thank Dr Dawn Bennett, Professor Glenys Parry and Debby Pickvance for their helpful comments. I’m thankful to the staff team for their ongoing work with the challenging clients and specifically to Steve Bucknell and Wendy Lowe for their invaluable contribution. I hope that Jack continues to experience positive improvements.
References
Davies, W. (2001) The Raid Manual. A Relentlessly Positive Approach to Working With Extreme Behaviour. APT Press: Leicester.
Dawson, D. F. (1988) Treatment of the Borderline Patient: Relationship Management Canadian Journal of Psychiatry 33 370-74.
Dunn, M. and Parry, G. (1997) A Reformulated Care Plan Approach to Caring for People with Borderline Personality Disorder in A Community Mental Health Service Setting. Clinical Psychology Forum 104 19-22.
Kerr, I. B. (1999) Cognitive Analytic Therapy for Borderline Personality Disorder in the Context of a Community Mental Health Team: Individual and Organisational Psycho dynamic Implications British Journal of Psychotherapy 15(4) 425-437.
Lloyd, J. and Williams, B. (2003) Reciprocal Roles and the ‘Unspeakable Known’ : Exploring CAT within Services for People with Learning Disabilities Reformulation Theory and Practice in CAT 19 19-25.
Nicholson, J. M. and Carradice, A. (2002) Clinical Psychology Provision for Inpatient Settings: A Challenge for Team Working? Clinical Psychology 18 25-30.
Prochaska, J. O. and DiClemente, C. C. (1986) The Transtheoretical Approach. Chapter in Norcross, J. C. Handbook of Eclectic Psychotherapy. Brunner Mazel : New York.
Ryle, A. and Kerr. I. B. (2002a) CAT in Various Conditions and Contexts. p 131-175. Chapter in Ryle, A. and Kerr, I. B. Introducing Cognitive Analytic Therapy. Principles and Practice. Wiley: Chichester.
Ryle and Kerr (2002b) The ‘difficult’ patient and contextual reformulation p 202-213. Chapter in Ryle, A. and Kerr, I. B. Introducing Cognitive Analytic Therapy. Principles and Practice. Wiley: Chichester.
Walsh, S. (1996) Adapting Cognitive Analytic Therapy to Make Sense of Psychologically Harmful Work Environments: British Journal of Medical Psychology 69 3-20.
Footnotes
1 Green care planning is based on the behavioural approach to putting all positive effort into appropriate (or green) behaviour and not into challenging (or red) behaviour. The approach emphasises building a constructive relationship with the client which works with their strengths and minimises their difficult behaviour (Davies, 2001). The green care plan pulls together the important aspects of the exits whilst also operationalising the development and maintenance of the alternative relationship or reciprocal role ‘respecting caring adult to respected, cared for adult’. It is intended to help guide staff on how to develop and maintain a positive working alliance using specific, concrete and practical information. The other exits from the SDRs are also described. For example, in Jack’s case, how to support him to go out, how to help build his social skills, how to break patterns of brooding, anger and anxiety.
2 CPA meetings are where the whole plan of care is reviewed by the multi disciplinary team and the client (if possible).
Dr Angela Carradice Clinical Psychologist
Forest Lodge, Sheffield
Full Reference
Carradice, A., 2004. Applying Cognitive Analytic Therapy to Guide Indirect Working. Reformulation, Autumn, pp.18-23.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
CAT Skills Training in Mental Health Settings
Freshwater, K. and Kerr, I., 2006. CAT Skills Training in Mental Health Settings. Reformulation, Summer, pp.17-18.
'Five Session CAT' Consultancy: Using CAT to Guide Care Planning with People Diagnosed within Community Mental Health Teams: Brief Summary Report
Dr Angela Caradice, 2013. 'Five Session CAT' Consultancy: Using CAT to Guide Care Planning with People Diagnosed within Community Mental Health Teams: Brief Summary Report. Reformulation, Winter, p.15,16,17,18,19.
Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services
Fisher, C., Harding, C., 2009. Thoughts on the Rebel Role: Its Application to Challenging Behaviour in Learning Disability Services. Reformulation, Summer, pp.4-5.
The experience of staff practising “Five Session CAT” consultancy for the first time: Preliminary findings.
Kate Freshwater, Jennifer Guthrie and Alison Bridges, 2017. The experience of staff practising “Five Session CAT” consultancy for the first time: Preliminary findings.. Reformulation, Summer, pp.59-62.
My Experience of Cognitive Analytic Therapy (CAT) within a Secure Forensic Setting
Moon, L., 2015. My Experience of Cognitive Analytic Therapy (CAT) within a Secure Forensic Setting. Reformulation, Winter, pp.12-15.
Other Articles in the Same Issue
Applying Cognitive Analytic Therapy to Guide Indirect Working
Carradice, A., 2004. Applying Cognitive Analytic Therapy to Guide Indirect Working. Reformulation, Autumn, pp.18-23.
CAT Publications Updates
Tony Ryle, 2004. CAT Publications Updates. Reformulation, Autumn, p.23.
Editorial
Mog Scott Stewart and Serena Nuttall, 2004. Editorial. Reformulation, Autumn, p.3.
Mindfulness and CAT
Wilde McCormick, E., 2004. Mindfulness and CAT. Reformulation, Autumn, pp.5-10.
Process Issues in Conducting CAT with Dissociative Identity Disorder
Kellett, S., 2004. Process Issues in Conducting CAT with Dissociative Identity Disorder. Reformulation, Autumn, pp.11-15.
Psycho-Social Checklist
-, 2004. Psycho-Social Checklist. Reformulation, Autumn, p.28.
Review of ‘The Self-Esteem Journal: Using a Journal to Build Self-Esteem’ by Alison Waines
Dower, C., 2004. Review of ‘The Self-Esteem Journal: Using a Journal to Build Self-Esteem’ by Alison Waines. Reformulation, Autumn, pp.29-30.
Review of "Writing Cures 'An Introductory Handbook Of Writing In Counselling And Therapy'"
Burns-Lundgren, E., 2004. Review of "Writing Cures 'An Introductory Handbook Of Writing In Counselling And Therapy'". Reformulation, Autumn, pp.30-31.
Thoughts on the Inner Dialogue Between a CAT Therapist and Karl - I am not a marxist - Marx
Welch, L., 2004. Thoughts on the Inner Dialogue Between a CAT Therapist and Karl - I am not a marxist - Marx. Reformulation, Autumn, pp.24-26.
Training Feedback
Sarah Lucas, Rachel Pollard and Anna Jellema, 2004. Training Feedback. Reformulation, Autumn, p.27.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.