Process Issues in Conducting CAT with Dissociative Identity Disorder
Kellett, S., 2004. Process Issues in Conducting CAT with Dissociative Identity Disorder. Reformulation, Autumn, pp.11-15.
I was approached at the 2004 CAT conference to write an article about the paper that I presented concerning a single case experimental design approach to conducting CAT with a client with severe dissociative psychopathology. Rather than repeat the outcome data (Kellett, 2004) here, it appeared a more interesting option to reflect upon the process issues in both conducting the case, receiving supervision, managing the follow-up appointments and the general issues relating to conducting CAT with clients within the dissociative disorders. Whilst discussing these issues I want to remain fairly pragmatic in approach, as this mirrors the style of the therapy conducted and appears most useful in the space allowed. If some of what I state seems obvious, then I apologise in advance. I don’t want to draw any grand conclusions or state any sweeping generalisations from a single case, but rather give people a feel for the journey that the client (in her many constituent parts), myself and my supervisor set out upon and eventually concluded. The numbered structure of the following material reflects Kluft’s (1993) general guiding principles for conducting psychotherapy with this client group, adapted specifically for CAT, with the intention of providing an impression of what it was like to conduct the case, particularly the post-SDR sessions.
Assessment issues and prose reformulation
The client was referred to the service after a long history of service involvement in other NHS Trusts, including five years of psychoanalytic psychotherapy in her most recent treatment exercise. Therefore the client was already able to describe in fairly intricate detail the means by which dissociative defences had initially been employed, the events which tended to promote dissociation and the manner in which she perceived fragmentation to her personality structure. I do not believe that the CAT conducted would have been as useful for a client whom was only partially aware of distinct and separate self-states and mirrors Pollock’s (2001) useful point that confusing multiplicity must be subjectively experienced by the client. In short, complete dissociative amnesia would be impossible for the client to describe and correspondingly impossible to map on the SDR. The client was able to provide the names, functions, roles and preferences for 53 dissociated identities (40 female and 13 male), which would qualify as evidence of a polyfragmented case (Ross, 1996). Phenomenological research indicates that the median number of dissociated identities varies between 8 (Ross, 1996) and 9 (Putnam et al, 1986). The client gave a history of chronic and gross levels of sexual, emotional and physical abuse in childhood, with aspects of such abuses continuing in adult relationships. In attempting the prose reformulation, what seemed most appropriate was modelling an accepting – accepted frame of reference for the symptoms and experiences that the client reported. Although this seems, clinically, the blindingly obvious thing to do, the client had many experiences of a rejecting – rejected type experiences with many previous contacts with mental health professionals, superimposed on pre-existent attachment type difficulties. Interestingly, the client would often also occupy a rejecting role in relation to her own history and memories and would often query whether she must have concocted the images she perceived in flashback and autobiographical/episodic memories. Therefore the prose reformulation attempted to be as descriptive as possible concerning what I was observing and of what the client was describing. To have direct, unequivocal and even-handed feedback on such issues seemed to deepen the therapeutic bond for the client. The prose reformulation therefore had as the first and primary target problem that of fragmentation, illustrating to the client the here and now basis of the therapeutic work and the importance of reducing dissociation between self-states. The client also reported that it was useful to comment specifically in the letter that her perception and response to the letter depended upon which self-state she happened to be occupying at that particular time – ranging from desire to be rescued to that of essentially being totally rejecting of the prose content.
Theory and Practice: producing the SDR
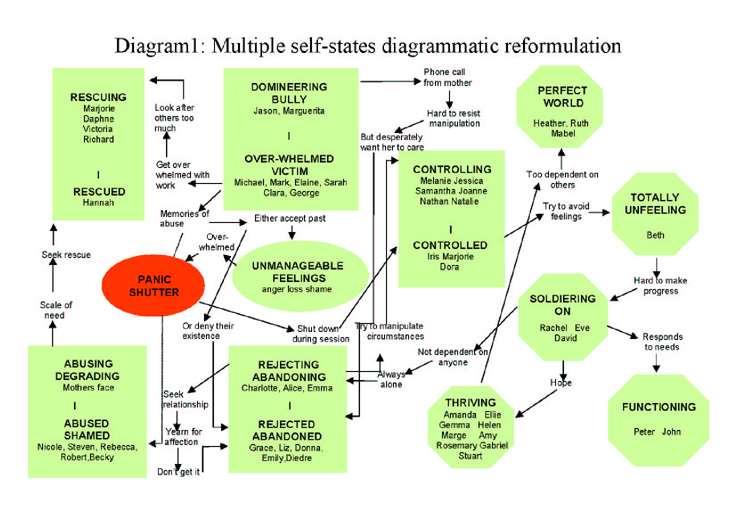
The Multiple Self States Model (MSSM – Ryle, 1997) appears tailor-made for conceptualising Dissociative Identity Disorder (DID) cases, due to the core assumptions and rationale for the model being founded upon notions of separate and fragmented self-states being maintained due to dissociation. Having the theory clear in my mind whilst assessing the client and in the sessions prior to producing the SDR, enabled the reformulatory work to flow with real purpose. Use of ‘maps’ such as the SDR are not uncommon in other therapeutic approaches with DID. Fine’s (1993, 1996, 1999) tactical-integrationist model (TIM) makes explicit use of maps of personality structure in the early phase of therapy. It is important however to draw a distinction between the CAT and the TIM maps. TIM maps appear to place sole emphasis on mapping the various identities and placing such identities on a diagram in relation to each other, in order to assess similarities, identify clusters and act as an ‘invitation’ to identities for therapeutic participation. The SDR produced in the case conducted was similar in terms to the TIM model in identifying clusters, but differed crucially in terms of the theoretical inclusion of reciprocal roles and procedural sequences between self-states. The SDR appeared to function as a real insight tool for the client, in terms of not only recognising the clusters, but for the first time understanding both how clusters reflected roles and how procedures linked fragmented self-states. The SDR is reproduced in diagram 1 for information. The reflective capacity (i.e. level 3 restriction in MSSM) of the client seemed enormously enhanced via the SDR, with the SDR also functioning as a containment tool of previous and numerous diffuse, confusing and seemingly contradictory experiences.
1. Frameworks and boundaries
As dissociative psychopathology appears the product of typically chronic boundary ignorance, violation and infringement, CAT with such clients obviously needs to maintain secure and firm boundaries. In the case I conducted, what seemed especially important was the treatment timeframe and how the client could make an informed decision about treatment. When I initially assessed the client, it was made crystal clear that the CAT would be 24 sessions, with four sessions of follow-up. The client was allowed to choose whether this was an option that she wished to pursue, as I stated that I could source long-term psychodynamic psychotherapy with a colleague should she wish. The client chose CAT, which seemed to clarify and make explicit the timeframe within which the treatment was to be conducted. The client’s awareness of the timeframe was always apparent even from the first session, with termination issues being live, apparent and acknowledged from the very first moments of therapy. The timeframe also within the CAT (i.e. three sessions to produce the prose reformulation) also appeared to facilitate effective boundaries, as it seems to prevent voyeuristic fascination with the clinical phenomena and rather corralled me into usefully observing and documenting self-states. Within the case it was necessary to adapt the style and content of the assessment, in order to reflect dissociative phenomena and symptomatology. During the assessment sessions and the sessions prior to producing the SDR, it was therefore necessary not only to join with the client in documenting a self-state, but also and crucially with the dissociated identities contained within reciprocal roles in particular self-states. The insight made in supervision that there were dissociative amnesias present both between and within self-states appeared to open up the field of clinical enquiry with the client in the attempt to map the system effectively. Again supervision was useful here, as an emphasis was placed upon the systemic nature of the intrapsychic phenomena, and the importance of producing a ‘good enough map of the whole’, rather than a piecemeal and fragmented SDR that would presumably only serve to reinforce separateness and lack of connectivity in the case.
2. Focus on achieving mastery
DID presents as a condition in which the client has little or no sense of subjective control over mental events and tends to hold the perception of themselves as housing many differing and often conflicted selves, which can at times confusingly assume executive control according to differing circumstance. Locus of control is internal, but tends to be splintered across identities, giving the client a global sense of helplessness in the face of often grossly contradictory means of relating and coping. The CAT conducted appeared useful as there was an explicit focus on mastery of present day proximal difficulties (whilst acknowledging the role of distal factors), rather than merely expecting such difficulties to fade as past events were processed. The client’s goodbye letter stated that she felt that she had really participated in the therapy, rather than being a dependant and passive recipient. The sense of participation seems based on the attempts to gain mastery via the therapeutic relationship, which was defined by activity based on reflective use of the SDR.
3. Establish and maintain therapeutic alliance
Although the outcome data did illustrate strong evidence of sudden gains in certain dissociative symptoms due to the introduction of certain CAT tools, such as the prose reformulation and the SDR, it seems that the effectiveness of these tools was only ‘activated’ within the context of the therapeutic relationship. The foundation stone of the therapeutic alliance allowed the therapy to contain a strong challenging component, as the client was challenged on repeating defensive and unhelpful patterns of relating from previous therapies and also on some of the basic dysfunctional assumptions, which contributed to snags. The balance of warmth and acceptance with challenge and confrontation appeared constantly shifting, and it was important to recognise that due to the fragmented personality structure what one dissociated identity may have found supportive, another identity may have found dismissive. Active reflection within the session was useful, whereby the client was asked to reflect on issues/events/achievements/difficulties, but also was invited to report on dissociated identities’ reactions and responses to the content of our conversations. As the therapy progressed, I felt increasingly able to ‘speak my mind’ to the client and felt a partner in a real on-going dialogue, rather than a ‘bit-part’ of frigid and stage-managed interaction. The follow-up sessions were often tricky to conduct due to the emphasis on review, which tends to take therapeutic alliance somewhat for granted. In this case it seemed that to ignore the alliance was to risk relapse.
4. Deal with buried trauma and affect
DID appears a presentation within which there are islands of dissociated and sequestered overwhelmingly negative affect. Within a reciprocal role and the identities that reflected poles of roles, there appeared apparent memories of past experiences and unexpressed associative affective responses. For the client, there appeared to be a particular clutch of distressing and previously unprocessed affect within the abusing-abused RR, with the SDR illustrating how the system was organised to both protect and maintain the unmanageable feelings. To work with the distressing affect, it was first necessary to work with the client regarding the dissociated identity that acted as ‘watch-person’ of an interpersonal alarm and safety system. Negotiating with the client about how to respect the previous need for such a system and discussions on how not to trigger the safety system appeared to engender trust, with the client subsequently being able to talk about feelings that she stated came from a ‘dank and dark cellar.’ The feelings within the abused role essentially focussed on characterological shame. The client requested in metaphor that I hold the door to the cellar open in order to allow the light in so that she would nor get lost and trapped. I never felt that the client had completely dealt with all the feelings in the abusing-abused role, but I did feel that the client had done enough in a 24-session therapy and the experience had taught the client that such work was possible, survivable and productive.
5. Reduce separateness
DID appears as a presentation within which the self is experienced as housing a variety of differing selves, often defined by conflict, but centrally by an overarching sense of confusion. The introduction of the SDR within the case was illustrated by a sudden gain in terms of a reduced sense of separateness. The SDR was constructed in the effort to name and contain all the various differing aspects of self on a single page, which in itself appeared to have a strong containing and insight-inducing effect on the client. Only when the client could see all the various aspects of herself together and connected in a system could any attempts at integration begin. Confusion appeared to be replaced at least to some extent by an ability to recognise and reflect on procedures – a core step in recovery using CAT.
6. Work to achieve congruence of perceptions
Perhaps common across attempts to help any person with any mental health problem is the need to be consistent in terms of communication across and within sessions. What appeared useful in the current case was that there was consistency between the various stages of the therapy, which reduced the possibility of any unhelpful confusing or conflicting communications. The goodbye letter built on the SDR, which built on the prose reformulation, which built on the therapeutic alliance. All the stages were bound by the common theme of integration. Integration was certainly not achieved in the current case (again, indexed experimentally) – but in terms of achieving congruence of perceptions across dissociated identities concerning the purpose of the intervention, then a common theme proved invaluable. The MSSM upon which the SDR was based seems particularly useful in visually formulating DID processes, as the model naturally lends itself to emphasising separateness between self-states.
7. Consistency
DID appears a mental health problem whose origins lie in the inconsistency of attachment figures, with complex systems of coping via dissociated identities emerging to survive the contradictions evident within and/or between attachment figures. Theoretically within the CAT model, no one reciprocal role procedure is championed over another, with an emphasis that positive change in roles, procedures, reflective capacities and so on, can all engender useful and positive change in the overall system. I feel the lack of championing certain self-states with regards to reciprocal roles gave an even handed approach to the content of the sessions. As my behaviour within sessions did not alter according to where on the SDR we were working, then this seemed to provide a strong message of consistency across dissociated identities. The stance taken by myself in the sessions was to remain as integrated and unified in my approach as possible. I can acknowledge that the client may not have experienced me as consistent due to vagaries of transference, but it was important for me to enable me to do the work to be as consistent in my responses and reactions as possible. Within the attempt to create consistency, supervision was centrally important as it modelled such a consistent approach. As I fretted and worried about process and relationships, my supervisor was responsive, but also channelled her utterances in consistent themes based explicitly in CAT theory.
8. Restore shattered basic assumptions
To have endured the abuse that many dissociative clients have had to bear leads to the generation of many trauma-based assumptions about the self (e.g. vulnerable, pathetic, victim etc.), the world (e.g. completely lacking in meaning, vengeful, changeable) and people in general (e.g. untrustworthy, disloyal, evil etc.). The work of the CAT obviously entailed attempts to build more balanced, compassionate and anxiety reducing assumptions about people, self and the world. The shattered assumptions in the client appeared to merge to produce a strong sense of herself as inherently bad and essentially rotten to the core. The client stated that to act in any way was essentially useless as she was, and always would be, a victim who acted as a lighthouse for the evil in others. Rather than challenging such assumptions outright (as I normally doggedly do), what appeared particularly useful in this case was to produce challenges based on the incontrovertible evidence of the progress made within the therapeutic relationship and associated gains made in the wider world. It seemed that being overtly supportive prior to any real progress was ineffective, as the client tended to be distrustful of any such statements. Progress, no matter how slight, (e.g. being able to stay with painful affect for a slightly longer length of time) seemed to provide a shared common foundation upon which challenges to shattered assumptions could be made. In her goodbye letter, the client stated that she had changed her perception of herself from pathetic victim to that strong survivor.
9. Minimise avoidable overwhelming experiences
As previously stated it seems impossible to develop DID without being exposed to a myriad of overwhelming experiences in the context of poor attachment. The pace of the CAT therefore was a crucial issue, especially given that fact that the international guidelines for treatment (ISSD, 1997) suggest at least six years of twice-weekly out-patient psychotherapy for averagely skilled therapists. It was important to recognise that despite 24 sessions realistically feeling like the proverbial drop in the ocean, it was still nevertheless a real and valid opportunity for the client and within the space that 24 sessions offers, it was still possible to pace certain stages of therapy. Supervision and related discussions about the client’s zone of proximal development served as a useful reminder of the disadvantages of premature, mistimed and over zealous interventions. Within sessions efforts were also made to pace discussions, so that by the final section of the 50 minutes, the client entered a stabilisation period. The pacing of the overall CAT was mainly concerned with providing the client with the support necessary to enable her to discuss intense feelings of shame, with additional time for reflection on the experience. It seems that to have rushed into the shame work centred within the abusing-abused reciprocal role would have likely been experienced as a re-enactment of the role itself.
10. Adopt an active, warm and flexible therapeutic stance
Within the history of the client, there were many painful examples of junctures where people who should have acted to protect the client simply stood back and allowed damage to occur. The client complained at assessment of a previous episode of therapy, during which she perceived the therapist as affectively blank and passive to the point of inertia and disinterest. Rather than the warm, active and receiving feeling of conducting the therapy being a stance or strategy, it rather felt an expression of the manner in which I like and hope to work with people. Although I’m aware that such personality variables do cast large therapeutic shadows in some cases, for the case discussed it felt like the right approach at the right time. The prose tools of CAT appeared to offer major opportunities with the client to model the feel of the overall therapy. The goodbye letters written by the client and myself were interestingly similar in content and structure. The warmness and closeness achieved seemed facilitated by activity rather than passivity.
Conclusions
The experience of working with the client was one that shared many characteristics of work with other chronic mental health problems that emphasised the shared common components of therapy across models and presentations, as it should do. However, the mechanisms of DID do appear to present quite distinct and unique challenges to the clinician. I often think to myself during therapy, as I say something to a client, how is this person experiencing this? During the current case, this reflection changed to, what does this system make of the stance that I’m taking? This appeared useful at the time, as it seemed to encourage being even handed, whilst being aware that the relationship was blatantly not one defined by equality. The benign yet active use of power seemed a somewhat new experience to the client. In conclusion, I hugely enjoyed conducting the case, but felt quietly relieved to finish the final follow-up session. It seemed really appropriate at this time to wave the client off into the world, confident that no harm had been done. With thanks to Debby Pickvance for her excellent supervision.
Stephen Kellett
Consultant Clinical Psychologist
Psychological Healthcare
Keresforth Centre
Barnsley S70 6RS
Stephen.Kellett@BarnsleyPCT.nhs.uk
References
Fine, C.G. (1993) A tactical-integrationalist perspective on multiple personality disorder. In R.P. Kluft & C.G. Fine (eds) Clinical Perspectives on Multiple Personality Disorder. Wsahington DC: American Psychiatric Press.
Fine, C.G. (1996). A cognitively based treatment model for DSM-IV DID. In L.K. Michelson & W.J. Ray (eds) Handbook of Dissociation. NY: Plenum Press.
Fine, C.G. (1999) The tactical-integration model for the treatment of DID and allied dissociative disorders. American Journal of Psychotherapy, 53, 361-376.
International Society for the Study of Dissociation. (1997). Guidelines for Treatment. ISSD, Northbrook: IL.
Kellett, S. (in press) The treatment of Dissociative Identity Disorder with Cognitive Analytic Therapy: Experimental Evidence of Sudden Gains. Journal of Trauma and Dissociation.
Kluft, R. (1993) Basic principles in conducting the psychotherapy of multiple personality disorder. In R.P. Kluft & C.G. Fine (eds) Clinical Perspectives on Multiple Personality Disorder. American Psychiatric Press; Washington DC.
Putnam, F.W. Guroff, J.J. Silberman, E.K. Barban, E.K. & Post, R.M. (1986). The clinical phenomenology of multiple personality disorder: Review of 100 recent cases. Journal of Clinical Psychiatry, 47, 285-293.
Pollock, P.H. (2001). A case of dissociative identity disorder. In P. Pollock (ed) Cognitive Analytic Therapy for survivors of sexual abuse. Wiley: Chichester.
Ross, C.A. (1996). DID: diagnosis, clinical features and treatment of multiple personality (2nd edition). New York: John Wiley.
Ryle, A. (1997). Cognitive Analytic Therapy and Borderline Personality Disorder: The Model and the Method. Wiley: Chichester.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Kellett, S., 2004. Process Issues in Conducting CAT with Dissociative Identity Disorder. Reformulation, Autumn, pp.11-15.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
States Characterisation Procedure (SCP) for supporting the reformulation of patients with borderline/dissociative features
Ryle, A., 2007. States Characterisation Procedure (SCP) for supporting the reformulation of patients with borderline/dissociative features. Reformulation, Winter, pp.9-11.
Journal Reviews Update Spring 2005
Ryle, A., 2005. Journal Reviews Update Spring 2005. Reformulation, Spring, p.19.
Generating Practice-Based Evidence for CAT
Marriott, M. and Kellett, S., 2007. Generating Practice-Based Evidence for CAT. Reformulation, Summer, pp.40-42.
Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.
CAT Effectiveness: A Summary
Quraishi, M., 2009. CAT Effectiveness: A Summary. Reformulation, Summer, pp.36-38.
Other Articles in the Same Issue
Applying Cognitive Analytic Therapy to Guide Indirect Working
Carradice, A., 2004. Applying Cognitive Analytic Therapy to Guide Indirect Working. Reformulation, Autumn, pp.18-23.
CAT Publications Updates
Tony Ryle, 2004. CAT Publications Updates. Reformulation, Autumn, p.23.
Editorial
Mog Scott Stewart and Serena Nuttall, 2004. Editorial. Reformulation, Autumn, p.3.
Mindfulness and CAT
Wilde McCormick, E., 2004. Mindfulness and CAT. Reformulation, Autumn, pp.5-10.
Process Issues in Conducting CAT with Dissociative Identity Disorder
Kellett, S., 2004. Process Issues in Conducting CAT with Dissociative Identity Disorder. Reformulation, Autumn, pp.11-15.
Psycho-Social Checklist
-, 2004. Psycho-Social Checklist. Reformulation, Autumn, p.28.
Review of ‘The Self-Esteem Journal: Using a Journal to Build Self-Esteem’ by Alison Waines
Dower, C., 2004. Review of ‘The Self-Esteem Journal: Using a Journal to Build Self-Esteem’ by Alison Waines. Reformulation, Autumn, pp.29-30.
Review of "Writing Cures 'An Introductory Handbook Of Writing In Counselling And Therapy'"
Burns-Lundgren, E., 2004. Review of "Writing Cures 'An Introductory Handbook Of Writing In Counselling And Therapy'". Reformulation, Autumn, pp.30-31.
Thoughts on the Inner Dialogue Between a CAT Therapist and Karl - I am not a marxist - Marx
Welch, L., 2004. Thoughts on the Inner Dialogue Between a CAT Therapist and Karl - I am not a marxist - Marx. Reformulation, Autumn, pp.24-26.
Training Feedback
Sarah Lucas, Rachel Pollard and Anna Jellema, 2004. Training Feedback. Reformulation, Autumn, p.27.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.