Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending
Mitzman, S. F., 2010. Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending. Reformulation, Summer, pp.26-30.
This article briefly illustrates a brief Cognitive Analytic Therapy (CAT) extended assessment and reformulation of a patient (identifying details have been altered to ensure anonymity) who is currently detained in High Secure Services. The collaborative sharing of contextual diagrammatic reformulation within multi-disciplinary teams within forensic settings is argued as essential practice as a means of developing a consistent understanding of the treatment needs of the patient. Contextual reformulation assists in highlighting factors associated with offending, making sense of difficult ward dynamics, and splits within the team and between professionals, and contributes to greater understanding of risk potential.
While the evidence base for CAT remains under-researched, the practice base for CAT is rapidly developing across a diverse range of clinical specialties, and is proving highly effective in the multi-disciplinary treatment, management and enhanced understanding, of ‘difficult to reach’ patients presenting with complex psychopathology. Pollock et al., (2006) elegantly describe the application of CAT conceptualisation, theory and intervention in forensic settings. CAT is currently provided across High, Medium and Low Secure Forensic Services within the U.K. and this growing recognition of the contribution of CAT is reflected in the establishment, very recently, of a national Special Interest Group in CAT and Forensic Practice, chaired by Phyllis Annesley, Consultant Clinical Psychologist, the first SIG meeting taking place at Rampton High Secure Services last year.
Forensic patients typically present with themes of early, severe deprivation, neglect and physical/sexual abuse, a ‘care’ history, identity disturbance, emotional volatility, chronic emptiness, experiences and fears of abandonment, substance misuse and chronic self harming – features strongly associated with extreme borderline characteristics and functioning. CAT provides a broad, and highly accessible, initial phase assessment/intervention which is complementary to, and can be combined with, formal risk and diagnostic assessment in forensic settings.
Individual and contextual reformulation is central to the practice of CAT, enabling the patient to re-tell their narrative, sourced (as much as possible) from the patient’s unique language, history, symbolism and metaphor, which is collaboratively formulated and negotiated with the patient, and those involved in providing care, as a means of enhancing shared insight, and consistent management and treatment goals within the teams and wider systems.
The reciprocal role repertoire of the forensic patient is frequently grossly restricted, damaged and damaging. The individual’s early pathological attachment experiences and restricted reciprocal repertoires are seen to ultimately contribute to, and are re-enacted in, the individual’s offending behaviour. Offending behaviour is ultimately relational and the motivation, contributory factors, and risk factors, are to be understood within the context of the offender’s reciprocal role repertoire and their relationship to the victim.
Forensic and/or borderline patients frequently experience an unstable sense of self characterised by confusing and extreme emotional states accompanied by high levels of arousal i.e. paranoia, fear, rage, anxiety and/or sexual tension, each state being associated with a specific repertoire of thoughts, affect and behaviour. State shifts may be characterised by varying levels of dissociation and the procedural pathway and rapid transition from one state to another, may act as precursors to violent offending and ward infringements. Rapid state shifts usually occur outside of the conscious awareness of the patient, and are confusing to both the patient and the clinician, and contribute to difficulties in making reliable clinical judgements relating to, and understanding, the ward management and the potential risk that the patient may pose while in detention, and in the wider community.
The contextual SDR seeks to assist the patient, clinician, and other care-staff, in making sense and meaning of the internal world of the patient’s conflicting and often, volatile state shifts and RRPs. The borderline patient lacks a whole and consistent understanding of him/herself, experiencing themselves and their immediate world as inconsistent, fragmentary and threatening. Such relational themes are frequently re-enacted and entrenched by the pathological ‘care’ systems which attempt to ‘treat and care for’ the patient and CAT is well-placed to ‘name’ and acknowledge the iatrogenic components of the individual’s psychopathology. Care-staff are frequently unintentionally and unwillingly ‘pulled into’ re-enacting unhelpful and ultimately collusive and polarised RRP re-enactments i.e. ‘punitive, controlling care-giving’ to ‘punished, crushed patient’, ‘special care-giving’ to ‘entitled patient’ etc. Frequently staff-patient relationships powerfully re-enact and collude with the early care-giving experiences of the patient and staff groups on the same ward find themselves polarised, experiencing extreme opposing feelings elicited by the same patient. In this way, iatrogenic factors frequently contribute to the exacerbation, and entrenchment, of the individual’s psychopathology. Thus the psychopathology of the patient is mirrored by the psychopathology of the system. In this way the confused and confusing, inconsistent and fragmented perceptions, and management, of the patient reflect the patient’s unstable sense of self and frequently contributes to highly conflicting notions of the patient’s clinical presentation, and their risk of re-offending.
Diagrammatic reformulation aims to provide the patient, CAT therapist, care team and ward staff with a systemic, contextualised holistic and integrated overview of the patient’s often bewildering and fragmented internal world. The process of developing a collaborative diagrammatic reformulation is frequently experienced by staff, and the patient, as a process akin to “putting together the jumbled pieces of their jigsaw puzzle to make a whole picture of themselves’. To maximise the clinical accuracy of the content of the SDR, in addition to patient self-report, corroborating information is drawn from;
- A trawl of the patient’s files; identifying pervasive relational themes from childhood and throughout the care system
- Consultation and reflective practice with the multi-disciplinary care team as a means of capturing the full range of polarised and competing feelings elicited in staff by the patient, and in the patient by staff
- Transference and counter-transference material
In summary, in forensic settings, an essential task of CAT reformulation is to identify, describe, contextualise and visually ‘bring alive’ the persistent, and unrevised, relational themes underpinning patterns of offending, ward based (parallel offending) re-enactments and patient-staff re-enactments. Contextual diagrammatic reformulation seeks to provide the patient, care-staff and ward with a shared, common, consistent and unifying language, understanding and therapeutic vision, to protect against ‘splitting’ and fragmentation. The SDR enables care-staff to recognise the potential for unhelpful and collusive staff-patient re-enactments. The reformulation process enables the patient (and staff) to recognise, ‘name’ and assume responsibility for the less desirable, unacceptable and frequently disavowed, violent and abusing aspects of themselves which underpin treatment and management and the patient’s offending and ward-based behaviour.
Case Summary and Diagrammatic Reformulation
Peter, aged 30, recently completed, this extended CAT assessment, which was his first, formal psychological intervention since his lengthy detention in High Secure Services. Peter was seen, by the author, on the ward, for 9 weekly sessions. Peter’s history and diagrammatic formulation is briefly summarised. All identifying details have been anonymised. Peter, and High Secure Services, have given permission for this case to be published.
Peter has been detained in High Secure Services for many years and has a Mental Disorder Classification of Psychopathic Disorder. Peter has a history of early maternal rejection and emotional exclusion, alleging that his father physically and sexually abused him from a very young age. Peter ‘managed’ his trauma, from childhood onwards, by self-medicating using copious substances. From age 13, Peter spent the majority of his life in children’s homes (where he alleges he was further sexually abused by care staff) and various forensic services. Peter has, from an early age, a history of aggressive, threatening and intimidatory behaviour and prolific offending primarily comprising robbery and violence. Peter also, has an early (and continuing) history of deliberate self harm, comprising severe cutting, over-dosing, and attempting to hang himself as a young adult which resulted in mild anoxia. Peter’s index offence is that of a life-threatening assault upon an emotionally vulnerable and frail older woman (for purposes of sensitivity and anonymity the specific details of this offence are not described in this paper). On the ward Peter was experienced by staff as either; ‘needy and exhausting and draining’ or ‘violent and intimidatory’ when his needs were not immediately met.
Peter describes, from early childhood and throughout his life, being exploited and manipulated by others. Peter has lived his life in a social environment characterised by community impoverishment and volatility, criminality and substance misuse. Peter presents as an immature, needy man with chronic low self-esteem and a history of forming premature emotional attachments to, and dependency upon, equally vulnerable women. Within the context of adult relationships, Peter describes being repeatedly exploited for money and drugs, and ultimately being rejected and betrayed by women (when he has no more to give materially) or abandoned by women (when he gives too much emotionally) resulting, on occasions, in Peter retaliating with violence – culminating in his index offence. It is also alleged that Peter has been violent towards a number of his partners’ children.
Peter describes feeling “mistrustful and lonely, numb and flat most of the time” and is noted on the ward to be pessimistic and often fearing the worst. Peter additionally describes a pervasive theme, throughout his life, of not being heard, listened to, or believed, by others.
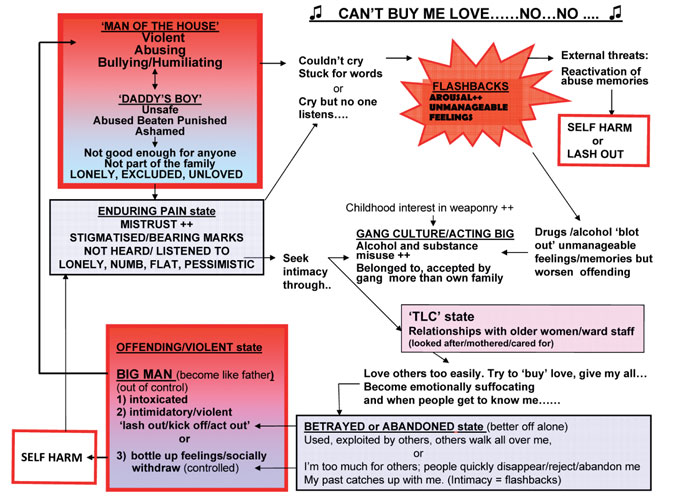
Development of the SDR
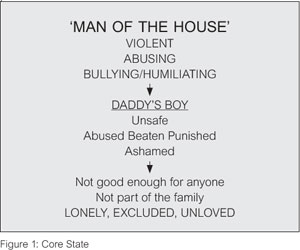
Figure 1: Core State
The Core State represents Peter’s childhood-derived reciprocal roles i.e. Peter’s father (man of the house), was a strict, authoritarian man who physically, emotionally and sexually abused, and humiliated, Peter. Peter experienced his father’s sexual abuse of him as having felt ‘chosen’ as ‘daddy’s boy’ while, at the same time, feeling ‘unsafe, abused, punished and ashamed’ and bearing the physical ‘marks’ and emotional stigmatisation of his abuse throughout his life. Peter’s mother was described as “a bag of nerves” and whom was distant and rejecting of Peter, while positively favouring his siblings. Abuse, exclusion and rejection contributed to Peter’s core experience of feeling ‘lonely, excluded and unloved’.
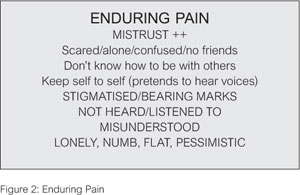
Figure 2: Enduring Pain
These early themes of abuse, punishment and neglect were (allegedly) repeated throughout Peter’s care in children’s homes contributing to his enduring pain (persisting through life); characterized by a powerful sense of ‘not being heard or listened to’ leaving him with a chronic sense of feeling ‘lonely, numb, flat and pessimistic’. Peter described these feelings deepening as a consequence of his mother, school, police, and prison workers, not believing, or being unwilling to act upon, Peter’s disclosures of sexual abuse at home and throughout the ‘care’ system.
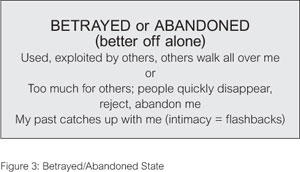
Figure 3: Betrayed/Abandoned State
Peter describes attempting to escape from his ‘enduring pain’ by seeking a sense of intimacy, inclusion and belonging, initially through gang culture. Peter described feeling closer to, and more accepted by, the gang than he ever had with his family. It is suspected that there was the potential however, given Peter’s vulnerability and immaturity, for the gang to also have exploited Peter (although this is denied). As part of the gang culture, Peter’s early involvement, and investment, in substances, weaponry, and violence, deepened. Peter’s use of drugs and alcohol escalated as a means of ‘blotting out’ his memories of abusive experiences and accompanying flashbacks, however, his increasing substance misuse escalated his violence and offending. Peter, later, continued to seek ‘intimacy, belonging and care’ through premature, and powerful, attachments to older women (often street-workers), with whom he would emotionally and materially ‘give his all’ attempting to buy their love with gifts, money and drugs. This dynamic is paralleled on the ward by Peter’s dependency, and his continual seeking of, ‘mothering and care’ from older female nursing staff. Peter’s potential to re-enact this pattern with the author during therapy was explored.
Peter’s indiscriminate, needy and suffocating style of attachment, preferring older women (i.e. partners/ward staff/CAT therapist, who “care more… look after me like a mum” powerfully positions him to be ‘betrayed; used, exploited’ or ‘abandoned; lonely and unloved’ by others, mirroring his relationship with his excluding and rejecting mother. On the ward, Peter is experienced as, at times, overwhelmingly needy, and highly sensitised, and reacting adversely, to perceptions of staff excluding him or favouring other patients (as his mother excluded him in preference to his favoured siblings). Peter, additionally described intimacy as dangerous (to self and others [in relation to his index offence]), activating ‘rejecting – rejecting’ reciprocal roles in that; either sexual closeness can elicit flashbacks of his early sexual abuse which is intolerable, leading Peter to ‘reject and flee’ the relationship, or paradoxically, when Peter became sexually intimate he felt compelled to disclose his history of assaultative behaviour towards children, thus he is ‘stigmatised’ (Enduring Pain) leading others (women/fellow patients) to reject him, either way he is ultimately left feeling lonely, numb and pessimistic.
Powerful feelings activated by experiencing being ‘used, betrayed and exploited’ by others or ‘rejected and abandoned’ by others (female partners/staff) led Peter to either; ‘bottling up his feelings, socially withdrawing, and self-harming’ or becoming ‘violent, intimidatory and lashing out’ (i.e. index offence/ward behaviours)
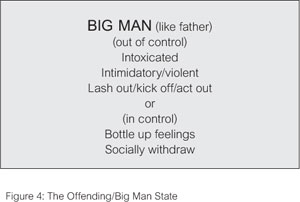
Figure 4: The Offending/Big Man State
when he behaves, and becomes like his father (Offending/Big Man state) i.e. ‘violent, abusing, bullying and humiliating’ to his victims/staff who are rendered ‘unsafe, abused, beaten, punished’.
Clinical recommendations arising from the CAT extended assessment and reformulation process.
Following CAT assessment and SDR reformulation it is the usual practice, within this High Secure Service, to continue to consult with ward and care staff, via the CAT therapist or Ward Liaison Psychologist, as a means of further exploring and developing the clinical themes arising from the CAT reformulation. Over time, with the continuing assistance of the CAT therapist and ward and multi-disciplinary staff, and in negotiation with the patient, behavioural/management exit strategies are further explored and incorporated into the SDR, which is intended as an evolving, rather than static, tool. The SDR is intended to ‘travel’ with the patient in their journey through conditions of lower security and/or community based settings, and the reformulation is refined as circumstances change.
Peter’s CAT reformulation highlights specific areas of his risk of violence to others; i.e. in sexual relationships, in which Peter is highly sensitised to themes relating to rejection, betrayal and abandonment thus contributing to his violence towards women. It is hypothesised that Peter’s alleged physical assaults on various partners’ young children may be motivated by jealousy associated with his sensitivity to feeling displaced, rejected and excluded (in the way in which his mother favoured Peter’s siblings) although Peter denies this. Currently Peter continues to minimise, the number and extent, of his assaults on women and children. Much of Peter’s denial appears to relate to his need to ‘be seen in a good light’, and his fear that acknowledgment of the extent of his aggression towards vulnerable others heightens the risk of further ‘stigmatisation’ and rejection. Continuing work is necessary to increase Peter’s insight into, and assume responsibility for, his violent offending, and to increase his capacity for victim empathy.
Peter’s chronic low self-esteem, neediness, dependency and emotional immaturity, render him susceptible to indiscriminating attachments to equally vulnerable others. These factors need to be addressed, in individual therapy, with a view to reducing the risk Peter poses to others in the community, and on the ward, when his relationships threaten to fail or his emotional needs are not met immediately. Similarly Peter needs to be able to develop more realistic expectations of others, and learn to manage and tolerate feelings of disappointment and frustration when his emotional needs cannot always be met. Very long term work is necessary to provide Peter with ‘ego-strength’ in order to address his pervasive (borderline) experience of loneliness, numbness and psychic isolation (Enduring Pain) which activates and ‘feeds’ his ‘addictive’ craving and need for constant ‘supplies’ of external reassurance and ‘love’ from ward staff. It is hoped that this work would assist in enabling Peter in strengthening his emotional resilience, and increasing his emotional autonomy and maturity, as such work is seen as essential in reducing Peter’s various risk to himself and his risk to others.
Finally, further investigation of Peter’s allegations of being sexually abused, while in care as a child, is essential, as good practice, and also to enable Peter to experience feeling ‘heard, understood and listened to’. Similarly further psychological work is needed to provide Peter with the opportunity to safely address the traumatic sequelae arising from his early physical and sexual abuse.
The contextual SDR was seen to increase staff’s psychological understanding of patient-staff re-enactments and provide a richer understanding of Peter’s offending pattern and risk potential. Many of the above treatment implications, arising from this first stage intervention, extended CAT assessment, are long-term and are being implemented by multi-disciplinary staff, in collaboration with the CAT therapist, in negotiating exit strategies that are workable for the patient, staff and the ward. Peter engaged well in the CAT work which was highly valued by the care staff. The formulation continues to inform day-to-day and longer term clinical management.
Susan Mitzman, Consultant Clinical Psychologist,
High Secure Services, Ashworth Hospital
Senior University Clinical Teacher, University of Liverpool
Address: susan.mitzman@merseycare.nhs.uk
Susan Mitzman is a Consultant Clinical Psychologist, with an enduring interest in working with complex presentations, and personality disorder, across a range of specialties. Susan was trained and supervised, by Tony Ryle from 1985-1987, prior to pursuing Clinical Psychology as a career. Since qualifying Susan has developed CAT practice within a number of services i.e. genito-urinary medicine, drugs and alcohol, adult mental health and eating disorders. For the last 6 years Susan has been working part-time on the Liverpool University Clinical Psychology Doctoral Training Programme where she takes a lead on disseminating CAT theory and practice to trainees, and in Ashworth High Secure Psychological Services, where she leads the CAT service.
References
Pollock, P.H. (2001). Cognitive Analytic Therapy for Adult Supervisors of Childhood Abuse; Approaches to Treatment and Case Management. Chichester: Wiley.
Pollock, P.H., Stowell-Smith, M., & Gopfert, M. (2006). Cognitive Analytic Therapy for Offenders: A New Approach to Forensic Psychotherapy. London and New York: Routledge.
Ryle, A. (1997). Cognitive Analytic Therapy and Borderline Personality Disorder: The Model and the Method. Chichester: Wiley.
Ryle, A., & Kerr, I.B. (2002). Introducing Cognitive Analytic Therapy: Principles and Practice. Chichester: Wiley.
Full Reference
Mitzman, S. F., 2010. Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending. Reformulation, Summer, pp.26-30.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
A Case Example of CAT with a Person who Experiences Symptoms of Psychosis
Dr Sara Morgan, 2018. A Case Example of CAT with a Person who Experiences Symptoms of Psychosis. Reformulation, Winter, pp.35-38.
My Experience of Cognitive Analytic Therapy (CAT) within a Secure Forensic Setting
Moon, L., 2015. My Experience of Cognitive Analytic Therapy (CAT) within a Secure Forensic Setting. Reformulation, Winter, pp.12-15.
Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management
Shannon, K., 2009. Using what we know: Cognitive Analytic Therapy's Contribution to Risk Assessment and Management. Reformulation, Winter, pp.16-21.
Helping service users understand and manage the risk: Are we part of the problem?
Crowther, S., 2014. Helping service users understand and manage the risk: Are we part of the problem?. Reformulation, Winter, pp.41-44.
Are we afraid to break tradition? Cognitive Analytic Therapy’s (CAT’s) contribution to the treatment of sexual risk
Sara Casado, 2018. Are we afraid to break tradition? Cognitive Analytic Therapy’s (CAT’s) contribution to the treatment of sexual risk. Reformulation, Winter, pp.26-31.
Other Articles in the Same Issue
Australia and New Zealand Unites Again; This Time to Consolidate the Promotion & Practice of CAT in the Region
McCutcheon, L., 2010. Australia and New Zealand Unites Again; This Time to Consolidate the Promotion & Practice of CAT in the Region. Reformulation, Summer, p.50.
Book Review: Self-Harm Assessment in Young People – A Therapeutic Assessment manual By Dennis Ougrin, Tobias Zundel and Audrey V. Ng Published by Hodder Arnold, 2010
Jenaway, Dr A., 2010. Book Review: Self-Harm Assessment in Young People – A Therapeutic Assessment manual By Dennis Ougrin, Tobias Zundel and Audrey V. Ng Published by Hodder Arnold, 2010. Reformulation, Summer, p.49.
Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending
Mitzman, S. F., 2010. Cognitive Analytic Therapy and the Role of Brief Assessment and Contextual Reformulation: The Jigsaw Puzzle of Offending. Reformulation, Summer, pp.26-30.
Confidentiality and Good Record Keeping in CAT Therapy - A Discussion Paper
Brown, H., 2010. Confidentiality and Good Record Keeping in CAT Therapy - A Discussion Paper. Reformulation, Summer, pp.10-12.
International CAT News
Potter, S., 2010. International CAT News. Reformulation, Summer, pp.51-52.
Letter from the Chair of ACAT
Westacott, M., 2010. Letter from the Chair of ACAT. Reformulation, Summer, pp.3-5.
Letter from the Editors
Hepple, J., Lloyd, J., 2010. Letter from the Editors. Reformulation, Summer, p.3.
Reflections on ACAT Relational Skills in CAT Supervision Course – December 2009
Coombes, J., Dunn, M., 2010. Reflections on ACAT Relational Skills in CAT Supervision Course – December 2009. Reformulation, Summer, pp.46-47.
The Development of a 12-Session CAT Therapy for Use in a Workplace Setting
Collins, J., 2010. The Development of a 12-Session CAT Therapy for Use in a Workplace Setting. Reformulation, Summer, pp.13-16.
The Development of a Cognitive Analytic Therapy (CAT) Relational Framework for Bipolar Disorder (BD)
Shannon, K. and Swarbrick, R., 2010. The Development of a Cognitive Analytic Therapy (CAT) Relational Framework for Bipolar Disorder (BD). Reformulation, Summer, pp.17-25.
The Political Sources of Reciprocal Role Procedures
Ryle, T., 2010. The Political Sources of Reciprocal Role Procedures. Reformulation, Summer, pp.6-7.
Therapeutic Change that is Dialogically Structured, Mediated by Signs, and Enabled by a Relationship – A Case Example
Bristow, J. and Reason, A., 2010. Therapeutic Change that is Dialogically Structured, Mediated by Signs, and Enabled by a Relationship – A Case Example. Reformulation, Summer, pp.31-33.
Thoughts and Experiences of the Application of Cognitive Analytic Therapy to Clinical Work with Adolescents
Mulhall, J., 2010. Thoughts and Experiences of the Application of Cognitive Analytic Therapy to Clinical Work with Adolescents. Reformulation, Summer, pp.34-36.
What Happens After “Happy Ever After�
Jenaway, A., 2010. What Happens After “Happy Ever After�. Reformulation, Summer, pp.8-9.
Will ACAT Join Other Professional Bodies in Calling for an End to the Detention of Families with Children?
Toye, J., 2010. Will ACAT Join Other Professional Bodies in Calling for an End to the Detention of Families with Children?. Reformulation, Summer, pp.47-48.
Words With Arrows The Benefits of Mapping Whilst Talking
Potter, S., 2010. Words With Arrows The Benefits of Mapping Whilst Talking. Reformulation, Summer, pp.37-45.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.