Metaprocedures in Normal Development and in Therapy
Hayward, M., McCurrie, C., 2008. Metaprocedures in Normal Development and in Therapy. Reformulation, Summer, pp.42-45.
Background
This article arose from a presentation we gave in May 2007, in the final term of our CAT practitioner course. During our training we had been introduced to the concept of metaprocedures but had been unable to find much literature on the subject. In our presentation we aimed to develop our understanding of the topic by identifying specific metaprocedures learnt during healthy childhood development and reflecting on the implications of damage to this process and how this is addressed in the therapeutic context.
Metaprocedures in their context
Through exploring the complex damage sustained by people with borderline personality disorder, Tony Ryle identified three distinct procedural levels, of which metaprocedures are the second (1). Ryle’s system offers a useful way of understanding normal processes of development, as well as how these can be disrupted through adverse childhood experiences, and we will therefore review the three levels briefly before going on to look at metaprocedures in more detail.
Level 1 procedures, or reciprocal role procedures (RRP’s), are perhaps those with which CAT therapists are most familiar. They are identified during reformulation through review of the client’s history, completion of the psychotherapy file and in-session interactions with the therapist. Described by role pairs such as ‘conditional/striving’ or ‘bully/martyr’, they develop from patterns of repeated interaction with early caregivers to become established ways of relating across a range of contexts.
Level 2 procedures, or metaprocedures, have a connective function, serving to mobilise and link level 1 procedures, as determined by the context and the individual’s aims and values. They are analogous to metalinguistic processes, which are described as the ‘superordinate cognitive structures that regulate the uses to which words and sentences are put’ (2). Ryle argues that a Bakhtinian perspective on the interpersonal nature of language organisation would suggest a close connection between metalinguistic processes and metaprocedures (1).
Level 3 procedures constitute conscious reflection by the individual on their own level 1 and 2 procedures. This self-reflection is represented by the ‘observing eye/I’ that is sometimes drawn on a Sequential Diagrammatic Reformulation, as an explicit recognition of the external observing stance.
Describing metaprocedures
As described above, metaprocedures are higher order procedures that provide a link between the immediate interpersonal interaction and the processes of self-reflection. Several features are important. Firstly, they act to connect and sequence level 1 procedures through offering a structure within which individuals can understand the interpersonal events around them and select appropriate responses. Secondly, this co-ordination of reciprocal role procedures occurs within the context of the individual’s value system, which is in itself in relationship to the broader socio-cultural context. Thirdly, they provide containment to difficult, affect-laden states, by offering explanations of why the states have arisen, and by suggesting appropriate interpersonal responses. Finally, they are largely unconscious and unreflected on.
An example may clarify this description. Consider a mother and her son talking about a playground fight in which he has been involved. As she talks to him, she tries to make sense of his behaviour and that of the others involved, on the basis of what intentional mental states, such as desires, feelings and beliefs, might have been operating. (This metaprocedure of mentalisation, which is a key part of emotional development, has been described more fully by Bateman and Fonagy (3).) The mother’s use of mentalisation allows her to understand not just the facts of what has happened, but the underlying emotional and cognitive processes of the children involved. She can then choose an appropriate response to her son. Through this, she will manage her own emotional response to the fight, modelling the ability to successfully contain affect and to reduce distress through appropriate practical action. This occurs in the context of her conscious beliefs and values about how children should treat each other and how adults should respond to children’s behaviour, in the context of wider influences such as the policies and culture of the child’s school. However, it is not a process of which she is likely to be consciously aware.
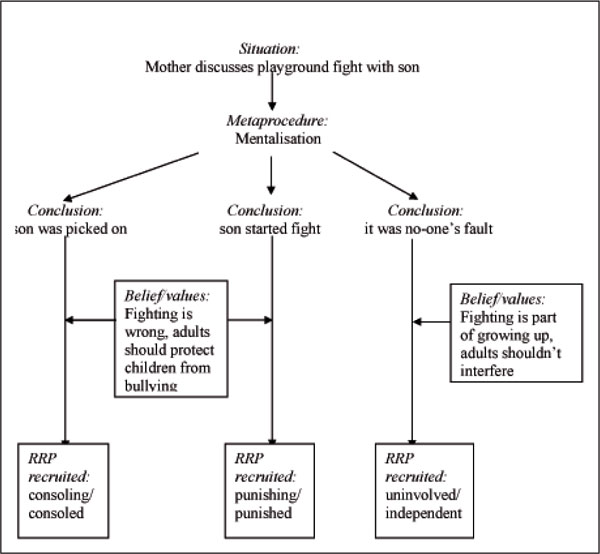
Figure 1 shows some of the possible outcomes of this interaction.
It is important to note that use of the same metaprocedure (mentalisation) can lead to the enactment of a range of different reciprocal roles, depending both on the context (the details about the fight) and the individual’s beliefs and values. Furthermore, it is possible that the outcome will prompt other interactions (for instance, conversations with the child’s peers, their parents or school staff), in which the mother will again use her skills in mentalisation to develop her understanding of the situation and choose appropriate responses. In conversation with her partner, or other family members, she may also discuss the situation and how she can best respond to her son. In this way the metaprocedure of mentalisation (level 2) can act both to recruit and organise reciprocal role procedures (level 1), and to stimulate conscious self-reflection (level 3).
Development of metaprocedures
As we have noted metaprocedures are largely unconscious processes, and like level 1 and 3 procedures they are initially acquired in the interpersonal context of early care. However, they continue to develop during childhood, and as the child increasingly engages in the world beyond the immediate family, the formal education system and wider society also influence their development. The moral and religious context of the family and social group will also shape the ends towards which developing metaprocedures are applied, through influencing the child’s values.
Both in the immediate context of the family and through broader social relationships, metaprocedures develop in the zone of proximal development, as described by Vygotsky. This zone is the gap between what can be done alone and what can be done with help from a more competent other, the dynamic area immediately beyond the child’s current independent competencies. In this zone the adult provides ‘scaffolding’ through which the child is able to develop new skills, before moving on to practise them with increasing independence. As Vygotsky put it, ‘what the child does with an adult today, she will do by herself tomorrow’. (4)
However, this development may be disrupted in several ways. In the absence of supportive adults, the child will lack the scaffolding that would normally support the development of procedures at all levels, and so will struggle to develop a healthy and flexible range of metaprocedures. The impact of neglect is more severe if experienced early in life, when the baby’s own sense of self is still developing and their independent resources are most limited. In addition, the development of metaprocedures relies heavily on the ability to organise experience into consistent patterns, from which predictions about the future can be made and strategies for responding to others developed. Consequently, when the child’s interpersonal experience is incoherent or contradictory, or when trauma induced dissociation disrupts the continuity of experience and memory, this lack of consistency seriously impairs the development of metaprocedures.
Damage often occurs at more than one procedural level, and these levels often interact, since damage at levels 1 and 2 makes it difficult to develop healthily at levels 2 and 3. As an example, if the available reciprocal role procedures are predominantly harsh or negative, it will be difficult for any metaprocedure to mobilise appropriate self-care when the individual is hurt or distressed. As Ryle identified, patients with borderline personality disorder have typically experienced damage at all three levels, and the characteristic partially dissociated self states may contain separate repertoires of metaprocedures, as well as reciprocal role procedures. This in turn makes the development of self-reflection more difficult.
Examples of metaprocedures in healthy development
Before examining the relevance of metaprocedures in the therapeutic context, it seems important to consider some of the metaprocedures acquired during healthy development. Although we suggest a number of examples in roughly chronological order, we do not assume these are acquired in an invariable sequence of linear development, or that the development of ‘later’ metaprocedures is always contingent on the mastery of ‘earlier’ ones. Rather, we anticipate that as progressive physical, cognitive and social development proceeds, and others continue to provide scaffolding, the child is able to develop a more diverse repertoire of metaprocedures and increasing flexibility in their use.
Babyhood
One important early metaprocedure, modelled from birth within the infant-carer dyad, is mirroring. This arises from the caregiver’s attunement to the baby’s emotions and constitutes a pre-verbal acknowledgement of the baby’s apparent mental state, in which the baby’s feelings are reflected back in a manageable form, for instance through the caregiver’s facial expression. This has links with Winnicott’s idea of ‘holding’ and Bion’s idea of ‘containment’ (5-7). Importantly, to be effective the mirroring should be both marked (meaning that the expression is exaggerated, making it easier for the baby to recognise) and congruent (meaning that the emotion reflected by the caregiver is the same as that expressed by the infant). When these criteria are met, the scaffolding is in place for the baby to progress within the zone of proximal development, and as a consequence the baby will gradually develop the ability to recognise and respond to its own mental state. Since the carer’s facial expression reflects the baby’s own internal emotional state, the baby develops a sense of self and agency. Where the baby is distressed, the carer’s initial mirroring is likely to lead to enactment of a soothing/soothed reciprocal role, for instance through feeding, changing or holding the baby, and the internalisation of this role lays the basis for the baby’s later self care.
Toddlerhood
A crucial metaprocedure that is characteristically developed in the infant-carer dyad during toddlerhood is that of boundary setting. The boundaries established, initially through the carer’s authority, set limits around acceptable level 1 procedures, prohibiting abusive, extreme or dangerous reciprocal roles. Thus, the toddler whose parent consistently tells them ‘no, don’t hit your sister, it’s not nice to hit people’ is presented both with explicit instruction on acceptable behaviour and with an underlying rationale, the authority of which will be reinforced and internalised through other moral guidance. The provision of consistent boundaries, either explicitly or implicitly, is a key factor in enabling the child to develop healthily. However, it is important to note that this level 2 procedure may organise level 1 procedures such as conditional/striving or punishing/punished in helpful or unhelpful ways.
Preschool children
From a Bakhtinian perspective, language is a key sign through which interpersonal activity leads to the internalisation of social meaning and cultural values. As the early non-verbal dialogue between carer and child is supplemented with verbal exchanges, each partner increasingly makes requests of the other. This mediates the development of an increasing mutuality and reciprocity in the relationship, in which each partner is able to ask for their own needs to be met, and to meet those of the other. On the one hand, the child becomes able to ask directly for things s/he wants, and the carer either fulfils the request (provider/recipient role), or sets a boundary. On the other, the carer’s requests of the child introduce the idea of ‘doing together’, and the metaprocedure of co-operation. As an example, the request to ‘help mummy do the shopping’ may lead to enactment of a number of different reciprocal roles, such as directing/compliant (the child picks up items the mother needs) or listening/listened to (the child suggests which flavour yoghurt to buy). The overall structure of their co-operation in completing the task successfully will determine the sequence in which the roles are recruited. Such co-operative exchanges are crucial in developing the social skills needed in larger groups, and for effective teamwork.
Early school years
During the early school years, the non-verbal metaprocedure of mirroring is increasingly supplemented by a verbal extension, in which emotional states are named and linked to external events. Thus the father who responds to his crying daughter with ‘Oh dear, you’re upset because you’ve lost your doll’ is modelling the early stages of mentalisation, explaining her behaviour (crying) by linking it to her mental state (upset) and suggesting the cause of her distress (losing her doll). As with all metaprocedures, this understanding also guides his response to her, in this case perhaps a joint search for the lost doll.
School years
As children’s abilities develop further, they increasingly explore and question the world around them. The resulting question-and-answer sessions with adults play a role in stimulating cognitive development, but also in social and emotional development and in the further development of mentalisation. Thus a child progresses from saying ‘I want more chocolate (to be met with either a fulfilment of the request or a boundary), to asking ‘Why can’t I have more chocolate?’ (enquiring about his mother’s behaviour towards him), to ‘Is Johnnie crying because he can’t have more chocolate?’ (theorising about the mental state behind his playmate’s behaviour) to ‘Why doesn’t Johnnie’s mum let him have more chocolate?’ (enquiring about the interaction between two others). Thus, he demonstrates an increasingly sophisticated ability to reflect on the mental states of others and use this to inform his own response.
As children continue to ask both why and how, the explanations of cause, effect and process they receive become more complex, cognitively and interpersonally, and as their ability to think more abstractly about other’s mental states develops, they become able to persuade or deceive others. This coincides with the move from, in Piaget’s terms, the pre-operational stage, to the concrete operational stage. In the latter, the social context of language use increasingly takes account of the mental states of others, as the child begins to be aware of what others do and do not know. Thus rather than crude requests being repetitively reiterated, the child becomes increasingly able to manipulate the effect they have on others’ mental states, and so persuade or deceive them, as well as use humour.
Adolescence
During healthy adolescence, two further important metaprocedures become more prominent, based on the wider range of skills the young person has now developed. Firstly, there is an increasing capacity for impulse control, encouraged through injunctions such as ‘count to ten before you react’, or ‘think before you speak’. The resulting metaprocedural inhibition of immediate level 1 responses creates a space in which self-reflection can occur (level 3), implying a more conscious, aim or value directed response. In this context, a second metaprocedure of problem solving may be invoked. This implies a process of identifying and evaluating problems, combined with a cognitive structure with which to generate and choose between a number of possible solutions, using resources available from self and others, and taking into account the likely consequences of the possible actions for all those involved. As an example, a young person may now respond to an insult from their sibling by inhibiting the initial impulse to hit out (metaprocedural inhibition of bully/victim role). Following this they may employ a problem solving metaprocedure to evaluate the interaction and select a response that furthers
their aims – even if this is still hitting their sibling, to teach them
a lesson!
Metaprocedures in therapy
During therapy, clients use scaffolding provided by the therapist within the zone of proximal development. As in childhood, the client initially observes procedures of all levels in use by the therapist, before beginning to employ them with support, and then developing increasing competence and autonomy in their use. As a result, where childhood damage has limited metaprocedural development, therapy offers an opportunity to experience and develop a fuller range of level 2 procedures, including through the introduction of new conceptual tools.
The therapeutic process itself, whatever the specific therapy, promotes development of many of the metaprocedures identified above. Recognition, naming of states of mind, and mirroring of affect by the therapist are carried out in many therapies, and might be seen as an essential prerequisite for a strong therapeutic alliance. These fundamental processes give the client a sense of being someone who ‘matters’, helping them to have a more solid sense of self and agency. In addition, they lay the foundation for the client to develop what may initially be a limited emotional vocabulary, acknowledge their pain and build up a more ‘compassionate mind’ (8), within which a soothing/distressed self-self role can be developed, balancing harsher and more self-critical roles. This process may be particularly important in clients who manage distress through self-harm, abnormal eating patterns or substance misuse, as they often lack healthy strategies to manage distress.
Boundary setting is also central, and therapists of all types will be familiar with the need to consistently attend to boundaries as clients test out the limits of the therapy situation. These limits may include how long and how frequently they can meet with the therapist, what types of support they can expect, and when the relationship will end. Where ‘acting out’ behaviour occurs inside or outside sessions the therapist will invite the client to join in thinking about it, aiming that the client should gradually learn to contain apparently unmanageable affect, and to control their first impulse to respond destructively or unhelpfully. In turn, this allows a process of understanding and attempting to solve problems experienced as unmanageable, overwhelming and unboundaried, using both the general metaprocedure of mentalisation, and the more specific tools of the individual therapeutic modality.
The metaprocedure of co-operation is also essential to an effective therapeutic relationship, expressed by Bordin in the agreed goal and allocated tasks of the therapeutic working alliance (9). Indeed, where therapy founders, this can often be traced to a failure to identify goals around which true co-operation can occur, resulting either in a pseudo-collaborative relationship, or overt tension. In the process of developing a shared understanding of the client’s problems, and hence promoting therapeutic co-operation, many therapies offer the client the metaprocedure of formulation. Arising from an exploration of the client’s story through the theoretical basis of the specific therapy, this offers a structure within which the client can understand their difficulties, contains unmanageable affect, and provides a link to conscious reflection on the procedural steps necessary to achieve positive change. Over the course of therapy, the therapist repeatedly models use of the formulation to understand both the generality and the specifics of the client’s problem, aiming that the client will become able to use the formulation metaprocedure independently as a way to understand and think about thoughts, emotions and actions. Indeed, as Bateman and Fonagy have pointed out, effective therapies require a therapeutic model that is coherent and comprehensible to both client and therapist (10). Once shared goals have been identified, it is the therapeutic model that offers the framework within which the tasks of client and therapist are elaborated, and specific metaprocedural tools employed. In the final section, we therefore discuss some of the specific metaprocedural tools used in CAT.
Therapy specific metaprocedures in CAT
In CAT, the Sequential Diagrammatic Reformulation (SDR, or ‘map’) demonstrates a therapy specific metaprocedure particularly clearly. In addition to representing level 1 procedures diagrammatically, the map offers client and therapist a way to understand the dynamics re-enacted in the therapeutic relationship (“where are we on the map?”), to identify repetition of unhelpful patterns, and to develop more healthy roles and procedures (e.g. listened to/understood versus rejected and angry/misunderstood). In addition, the prose reformulation (‘letter’) offers a narrative explanation of the client’s difficulties, modelling a compassionate response to painful early experience. This reworking of the personal narrative allows embodiment of personal and social meaning and links experiences to promote integration, so that like the SDR, the letter both offers a new metaprocedure and promotes self-reflection (level 3). In addition, the procedural sequence model (PSM) fulfils a similar metaprocedural function to the SDR with regard to a single procedure, explaining the maintenance of the problem, and offering points for intervention to promote change.
We suggested above that problem solving is an important metaprocedure developed during adolescence, and a number of therapeutic ‘problem solving’ techniques can offer structures to understand events and select appropriate, healthy responses. These include cognitive techniques, self-monitoring diaries and explicit teaching of problem solving strategies. This may lead on to an exploration of techniques for emotional management, or of social skills such as negotiation. Use of metaphor and story in therapy may also offer a powerful route into a more affect laden domain, which may prove helpful to clients who tend towards an intellectualisation of their problems. Using metaphor may promote an increasing recognition and understanding of emotional states and can aid the development of ‘exits’ from the client’s map. This is often summed up through reference to an episode when a new relationship pattern was in evidence, this episode becoming a metaphor of the change occurring during therapy. In this sense, metaphor itself can be a vital therapeutic metaprocedure, offering a way of understanding events, containing affect, and moving towards more healthy patterns of relating.
Summary
Many clients come to therapy with early experiences that have left them not only with an inflexibly applied and restricted range of reciprocal role procedures (level 1), but also with a limited range of tools to connect and sequence their procedures (level 2), and limited ability to self-reflect (level 3). Through the consistency and predictability of the therapeutic relationship, as well as the specific tools of therapy, clients are offered an opportunity to develop procedures at all of these levels, and gains made in therapy may be as much about development of metaprocedures and self-reflection as about the establishment of new reciprocal roles. Indeed, increased flexibility in the use of reciprocal roles will necessarily entail a development of metaprocedures and self-reflection. However, for this to occur successfully, the therapist must remain within the client’s zone of proximal development.
We conclude that when therapy seems stuck, it may be useful not only to review the reciprocal roles in operation, but also the range of metaprocedures employed by the client. By ensuring that interventions remain close to the client’s current level of functioning, the therapist can offer effective therapeutic scaffolding and hence create a realistic possibility for change.
Marianne Hayward is a Consultant Psychiatrist in general adult psychiatry and CAT practitioner trainee, and Caroline McCurrie is a Specialist Registrar in psychotherapy and CAT practitioner trainee.
Situation:
Figure 1: Example of metaprocedure in use: Mother discusses playground fight with son’ (see above)
Reference List
(1) Ryle A, Leighton T, Pollock P. Cognitive analytic therapy and borderline personality disorder: The model and the method. 1997.
(2) Donald M. Origins of the modern mind: Three stages in the evolution of culture and cognition. 1991.
(3) Bateman AW, Tyrer P. Psychological treatment for personality disorders. Adv Psychiatry 2004 Sep 1;10(5):378-88.
(4) Vygotsky L. Mind in society: The development of higher psychological processes. Cambridge, MA: Harvard University Press; 1978.
(5) Winnicott DW. The Theory of the Parent-Infant Relationship. Int J Psychoanal 1960;41:585-95.
(6) Bion WR. Attacks on linking. Int J Psychoanal 1959;40:308-15.
(7) Bion WR. Learning from experience. London: Heinemann; 1962.
(8) Gilbert P. Compassion: Conceptualisations, research and use in psychotherapy. 2005.
(9) Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy: Theory, Research & Practice 1979;16(3):252-60.
(10) Bateman AW, Fonagy P. Effectiveness of psychotherapeutic treatment of personality disorder. Br J Psychiatry 2000 Aug 1;177(2):138-43.
Full Reference
Hayward, M., McCurrie, C., 2008. Metaprocedures in Normal Development and in Therapy. Reformulation, Summer, pp.42-45.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Change of State: Learning How To Manage Unmanageable Feelings and States
Bristow, J., 2006. Change of State: Learning How To Manage Unmanageable Feelings and States. Reformulation, Summer, pp.6-7.
Book Review of: Beatrice Beebe and Frank Lachmann (2002). Infant Research and Adult Treatment: Co-constructing Interactions. Published London: Analytic Press.
Lloyd, J., 2009. Book Review of: Beatrice Beebe and Frank Lachmann (2002). Infant Research and Adult Treatment: Co-constructing Interactions. Published London: Analytic Press.. Reformulation, Summer, pp.34-35.
A Hopeful Sequential Diagrammatic Reformulation
Bradley, J., 2012. A Hopeful Sequential Diagrammatic Reformulation. Reformulation, Summer, pp.13-15.
Attachment, The Body and Trauma
Diamond, N., 2005. Attachment, The Body and Trauma. Reformulation, Autumn, pp.25-26.
Working within the Zone of Proximal Development: Reflections of a developing CAT practitioner in learning disabilities
Frain, H., 2011. Working within the Zone of Proximal Development: Reflections of a developing CAT practitioner in learning disabilities. Reformulation, Winter, pp.6-9.
Other Articles in the Same Issue
CAT Used Therapeutically and Contextually
Murphy, N., 2008. CAT Used Therapeutically and Contextually. Reformulation, Summer, pp.26-30.
Catch up with CAT
Potter, S., Curran, A., 2008. Catch up with CAT. Reformulation, Summer, p.54.
Clinical Implications for the Pregnant CAT Therapist
Knight, A., 2008. Clinical Implications for the Pregnant CAT Therapist. Reformulation, Summer, pp.38-41.
Consent to Publish in Reformulation
Jenaway, A., Lloyd, J., 2008. Consent to Publish in Reformulation. Reformulation, Summer, p.7.
Cuckoo Lane
Selix, M., 2008. Cuckoo Lane. Reformulation, Summer, p.6.
How to Enjoy Writing a Prose Reformulation
Wilde McCormick, E., 2008. How to Enjoy Writing a Prose Reformulation. Reformulation, Summer, pp.16-17.
Integration of Cognitive Analytic Therapy Understandings
Ruppert, M., Birchnall, Z., Bruton, C., Christianson, S., 2008. Integration of Cognitive Analytic Therapy Understandings. Reformulation, Summer, pp.20-22.
Is CAT an Island or Solar System?
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.
Letter from the Chair of ACAT
Westacott, M., 2008. Letter from the Chair of ACAT. Reformulation, Summer, pp.3-4.
Letter from the Editors
Elia, I., Jenaway, A., 2008. Letter from the Editors. Reformulation, Summer, p.3.
Metaprocedures in Normal Development and in Therapy
Hayward, M., McCurrie, C., 2008. Metaprocedures in Normal Development and in Therapy. Reformulation, Summer, pp.42-45.
Plugging in and Letting Go: the Use of Art in CAT
Hughes, R., 2008. Plugging in and Letting Go: the Use of Art in CAT. Reformulation, Summer, pp.9-10.
Service Innovation
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.
Silence in Practice
Harvey, L., 2008. Silence in Practice. Reformulation, Summer, pp.11-13.
The ‘Human Givens’ Fast Trauma and Phobia Cure
Jenaway, A., 2008. The ‘Human Givens’ Fast Trauma and Phobia Cure. Reformulation, Summer, pp.14-15.
The Body in Dialogue
Burns-Lundgren, E., Walker, M., 2008. The Body in Dialogue. Reformulation, Summer, pp.18-19.
The Development of the Sequential Diagrammatic Reformulation
Parkinson, R., 2008. The Development of the Sequential Diagrammatic Reformulation. Reformulation, Summer, pp.33-37.
The States Description Procedure
Hubbuck, J., 2008. The States Description Procedure. Reformulation, Summer, pp.46-53.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.