Service Innovation
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.
Introduction
Most child and adolescent mental health services would like to have some access to psychodynamic therapy. However, child therapists trained in psychodynamic therapy are in short supply, and offering long term therapy is not always practical or cost effective. We describe a pilot to see if offering Cognitive Analytic Therapy within a CAMH service is a helpful alternative.
Cognitive Analytic Therapy is a brief therapy, usually 16 sessions, which has developed as an integration between cognitive behaviour therapy and psychodynamic therapy. It has been used mainly in adults and old age services and in naturalistic studies has shown an effect size similar to other psychotherapies (Dunn et al, 1997, Sutton and Hepple). It has been promoted as a particularly useful therapy for those with borderline personality disorder (Ryle and Golynkina, 2000)). Generally for those with more severe personality difficulties, the recommendation is to offer 24 sessions. There are a number of controlled trials underway and there has been one randomised controlled trial of cognitive analytic therapy in 15 to 18 year olds with risk factors for borderline personality disorder in Melbourne, showing that it is more effective than treatment as usual for this group (Chanen et al, 2006).
In the pilot we were interested in whether the therapeutic tools of CAT, the Reformulation letter, Diagram, Rating sheets and Goodbye letter, could be used with adolescents in the same way as with adults, and whether they would be helpful and meaningful to them. We were also interested in how helpful the young person found the therapy overall.
Method
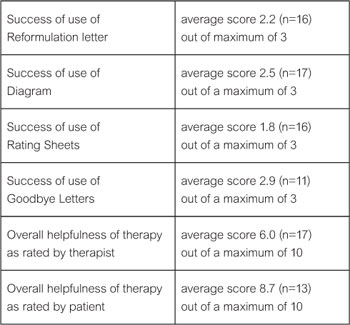
The authors were working in CAMH services in Huntingdon and Cambridge and took on young people aged between 14 years and 18 years for standard cognitive analytic therapy. Referrals were from general practice, other CAMH professionals and some from adult mental health services, of young people who had problems which appeared to be mainly in the area of their interpersonal relationships. At the end of therapy, the therapist filled in a form with demographic details, information about previous treatment, previous time in care, and current social and educational circumstances. Therapists were then asked to rate according to a 4 point scale how helpful each of the four tools of CAT (Reformulation letter, Diagram, Rating sheet and Goodbye letter) had been:
Scale
0 = not used as did not seem possible/appropriate
1 = used but the patient did not understand it/like it
2 = used and the patient seemed to understand it and find it somewhat useful
3 = used and patient found it very useful eg. used it during sessions
At the final session, patients were asked to rate on a visual Likert scale of 0 to 10 how helpful the CAT therapy had been and the therapist did a similar rating (0=not at all helpful, 5=somewhat helpful and 10=very helpful). Patients who dropped out of therapy were sent a brief questionnaire, and stamped addressed envelope, asking them to rate the therapy on the same scale and also indicate why they had left therapy earlier than planned.
Results
Seventeen patients were included in the pilot, with an average age of 15.9 years (range from 14 to 18). Five (29%) were boys, all but two (12%) had attended mainstream school, with four (24%) having spent some time being looked after by social services. Fifteen (88%) were thought to have primarily personality difficulties, while 2 (12%) had primarily depressive illness. Thirteen (76%) had a history of self harm. Ten (59%) had received previous psychiatric treatment from specialist CAMH services. Patients attended for an average of 14 sessions (range 3 to 22) and 8 (47%) of patients ended therapy in an unplanned way. Four of these drop outs subsequently sent back rating sheets.
The results of the scores are shown in table 1.
Discussion
With nearly all patients it was possible to use the standard tools of CAT. In working with adolescents it is important to work hard at engaging them in the therapy process in the first few sessions and this often meant spending quite a bit of time explaining the ideas behind CAT and the reason for taking such a broad view of the young person’s personality and situation, rather than just the presenting problem. We had thought that the Reformulation letter might be too overwhelming for adolescents but actually they seemed less intensely affected than adults. Perhaps because there was less historical information to gather and they are, in general, less focused on the more distant past, and much more focused on what happened last night, and what is going to happen tomorrow. One patient dropped out before receiving the Reformulation letter but all the others collaborated in making the letter a joint understanding of their difficulties. Most patients did not refer to the letter again but a few kept it and used it as something to read through when they felt down or confused. This was reported as being helpful in reminding them of where their difficulties arose, and what they were doing to overcome them. We were conscious that some of the reformulation letters would be seen by parents and so we worked hard to make sure that they were not too critical of parents and presented more of an understanding of the parent’s own difficulties. There were no complaints from parents about the reformulation letters.
The diagram seemed to work well with all the young people, it was often possible to start drawing the diagram together in the first or second session. It seemed important to make the diagrams more interesting and more personalised. For example, by creating a visual representation of the roles, using images rather than just words, or making the whole thing into a picture. This seemed to help the young person take ownership of the diagram and meant they were more likely to use it.
The use of the rating scales seemed least useful with adolescents, it was difficult to focus down to specific problems and aims, and some did not seem to like rating themselves. Goodbye letters were successful for those who stayed to the end of therapy and many wrote their own letter back to the therapist.
The adolescents rated the helpfulness of therapy very highly, although this could partly be due to a wish to please the therapist, as the rating took place at the final session rather than anonymously at a later time. Including those who had dropped out of therapy early, but returned a feedback form, did not reduce the overall rating. All but one of these drop outs said that they had dropped out because of practical difficulties getting to the sessions. We do not know what the 4 patients who did not return a questionnaire thought of the therapy, or their reasons for dropping out.
Clinical Implications
It does seem possible to use standard Cognitive analytic therapy with adolescents from 14 years old. Even young people with quite significant problems and risky behaviour seem able to use the tools of the therapy and find them helpful. The high drop out rate of 47% is fairly usual for studies of psychotherapy with adolescents (Wierzbicki, M., and Pekarik, G.,1993), and at least some of those seem to have dropped out due to practical difficulties in attending rather than to dissatisfaction with the therapy. Further work needs to be done using more objective measures, and a larger sample size, to see how effective the therapy is.
References
Chanen, A. et al (2006). A randomised controlled trial of psychotherapy for early intervention for borderline personality disorder. Acta Neuropsychiatrica, 18 (6) 319.
Dunn, M., Golynkina, K., Ryle, A., and Watson, J.P. (1997). A repeat audit of the cognitive analytic clinic at Guy’s Hospital. Psychiatric Bulletin, 21, 1-4.
Dunn, M. and Parry, G.D. (1997). A formulated care plan approach to caring for borderline personality disorder in a community health setting. Clinical Psychology Forum, 104, 19-22.
Ryle, A. and Golynkina, K. (2000). Effectiveness of time-limited cognitive analytic therapy of borderline personality disorder; Factors associated with outcome. British Journal of Medical Psychology, 73, 169-177.
Ryle, A. and Kerr, I.B. (2003). Introducing Cognitive Analytic Therapy, Principles and Practice, John Wiley & sons.
Wierzbicki, M. and Pekarik, G. (1993). A metaanalysis of psychotherapy dropout. Professional Psychology: Research and Practice, 24, 190-195
Dr Alison Jenaway, Consultant Psychiatrist in Psychotherapy, CAMH, Newtown Centre, Nursery Road, Huntingdon.
Debbra Mortlock, Clinical Psychologist, CAMH, Brookside Family Consultation Clinic, Trumpington Road, Cambridge.
 Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!
Petition to NHS England - The Case for Funding Training in the NHS 2021
Alert!ACAT's online payment system has been updated - click for more information
Full Reference
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
The CAT Articles Review
Knight, A., 2009. The CAT Articles Review. Reformulation, Summer, p.32.
Using Cognitive Analytic Therapy with parents: some theory and a case report
Jenaway, A., 2007. Using Cognitive Analytic Therapy with parents: some theory and a case report. Reformulation, Winter, pp.12-15.
Research Into the Use of CAT Rating Sheets
Coombes, J., Taylor, K. and Tristram, E., 2009. Research Into the Use of CAT Rating Sheets. Reformulation, Winter, pp.28-29.
Audit of Factors Predicting Drop Out from Cognitive Analytic Therapy Kerrie Channer and Alison
Channer, K., Jenaway, A., 2015. Audit of Factors Predicting Drop Out from Cognitive Analytic Therapy Kerrie Channer and Alison. Reformulation, Winter, pp.33-35.
CAT Effectiveness: A Summary
Quraishi, M., 2009. CAT Effectiveness: A Summary. Reformulation, Summer, pp.36-38.
Other Articles in the Same Issue
CAT Used Therapeutically and Contextually
Murphy, N., 2008. CAT Used Therapeutically and Contextually. Reformulation, Summer, pp.26-30.
Catch up with CAT
Potter, S., Curran, A., 2008. Catch up with CAT. Reformulation, Summer, p.54.
Clinical Implications for the Pregnant CAT Therapist
Knight, A., 2008. Clinical Implications for the Pregnant CAT Therapist. Reformulation, Summer, pp.38-41.
Consent to Publish in Reformulation
Jenaway, A., Lloyd, J., 2008. Consent to Publish in Reformulation. Reformulation, Summer, p.7.
Cuckoo Lane
Selix, M., 2008. Cuckoo Lane. Reformulation, Summer, p.6.
How to Enjoy Writing a Prose Reformulation
Wilde McCormick, E., 2008. How to Enjoy Writing a Prose Reformulation. Reformulation, Summer, pp.16-17.
Integration of Cognitive Analytic Therapy Understandings
Ruppert, M., Birchnall, Z., Bruton, C., Christianson, S., 2008. Integration of Cognitive Analytic Therapy Understandings. Reformulation, Summer, pp.20-22.
Is CAT an Island or Solar System?
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.
Letter from the Chair of ACAT
Westacott, M., 2008. Letter from the Chair of ACAT. Reformulation, Summer, pp.3-4.
Letter from the Editors
Elia, I., Jenaway, A., 2008. Letter from the Editors. Reformulation, Summer, p.3.
Metaprocedures in Normal Development and in Therapy
Hayward, M., McCurrie, C., 2008. Metaprocedures in Normal Development and in Therapy. Reformulation, Summer, pp.42-45.
Plugging in and Letting Go: the Use of Art in CAT
Hughes, R., 2008. Plugging in and Letting Go: the Use of Art in CAT. Reformulation, Summer, pp.9-10.
Service Innovation
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.
Silence in Practice
Harvey, L., 2008. Silence in Practice. Reformulation, Summer, pp.11-13.
The ‘Human Givens’ Fast Trauma and Phobia Cure
Jenaway, A., 2008. The ‘Human Givens’ Fast Trauma and Phobia Cure. Reformulation, Summer, pp.14-15.
The Body in Dialogue
Burns-Lundgren, E., Walker, M., 2008. The Body in Dialogue. Reformulation, Summer, pp.18-19.
The Development of the Sequential Diagrammatic Reformulation
Parkinson, R., 2008. The Development of the Sequential Diagrammatic Reformulation. Reformulation, Summer, pp.33-37.
The States Description Procedure
Hubbuck, J., 2008. The States Description Procedure. Reformulation, Summer, pp.46-53.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify
Help
This site has recently been updated to be Mobile Friendly. We are working through the pages to check everything is working properly. If you spot a problem please email support@acat.me.uk and we'll look into it. Thank you.